PD26-01: En-bloc versus conventional transurethral resection of bladder tumors: single-center prospective randomized trial
Saturday, May 14, 2022
1:00 PM – 1:10 PM
Location: Room 252
Andrea Gallioli, Pietro Diana*, Matteo Fontana, Angelo Territo, Alberto Piana, Ferran Algaba, Óscar Rodriguez-Faba, Asier Marcadé, Alejandra Bravo, Antonio Rosales, Josep Maria Gaya, Joan Palou, Alberto Breda, Barcelona, Spain
Introduction: Transurethral resection of bladder tumor (TURBT) is considered the gold standard in the diagnosis and risk stratification bladder cancer (BC). En-bloc resection of bladder tumor (ERBT) has been proposed to improve resection quality. Recently, the International Collaborative Consensus Statement on ERBT underlined the lack of high-quality prospective studies precluding the achievement of solid conclusion on ERBT. The aim of our study is to compare TURBT and ERBT in pathological diagnosis, surgical, and oncological outcomes.
Methods: This study is a prospective, randomized trial enrolling patients diagnosed with BC and undergoing endoscopic intervention. Inclusion criteria were: tumor size of =3 cm, and =3 lesions, and no sign of muscle invasion and/or ureteral involvement. The primary outcome is the staging of BC. Secondary outcomes included T1 substaging (microstaging systems T1a/b/c), intraoperative complications, rate of adjuvant treatment, postoperative complications, oncologic outcomes. With an a and ß risk of 2.5% and 20% with a non-inferior difference of 5% en the rate of detrusor muscle presence, a total of 300 subjects were included in the study with 1:1.5 treatment allocation for ERBT. The trial (NCT04712201) was approved by the Institutional Review Board (2017/09c).
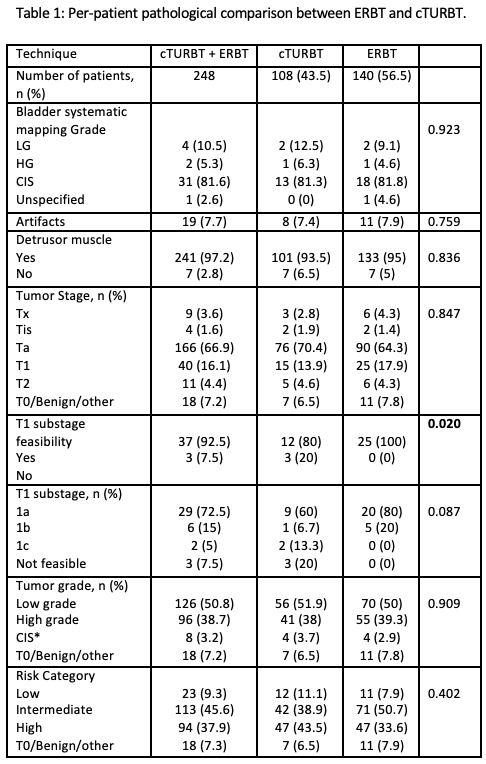
Results: From 03/2018 to 06/2021, 300 patients met inclusion criteria and 248 (82.7%) of these were underwent the assigned intervention. 108 (43.5%) and 140 (56.5%) patients were submitted to TURBT and ERBT. Pre-operatively, the populations were comparable. Table 1 shows the pathological results per patient. The rate of Tx was comparable (2.8% TURBT vs 4.3% ERBT). T1 substaging was feasible in 80% TURBT vs 100% ERBT (p=0.02). The rate of obturator nerve reflex and perforation were comparable (both p=0.2). In patients candidate to adjuvant treatment, the instillation was performed in 86% and 94% in TURBT and ERBT (p=0.1). Clavien-Dindo >2 complications were 2.8% vs 4.3% for TURBT and ERBT. Surgical, irrigation, and catheterization time were all comparable (all p>0.05). Recurrence rate at a median follow-up of 12 months (7-25) was 17.6% vs 12.9% in TURBT and ERBT (p>0.1).
Conclusions: ERBT is non-inferior to TURBT in pathological, surgical, and short term oncological outcomes. ERBT reported a higher rate of T1 substaging feasibility compared to TURBT. This is the largest randomized study in this setting.

.jpg)
.jpg)