PD26-06: Adjuvant chemotherapy plus radiotherapy versus chemotherapy alone for locally advanced bladder cancer after radical cystectomy.
Saturday, May 14, 2022
1:50 PM – 2:00 PM
Location: Room 252
John Ernandez*, Sumedh Kaul, Aaron Fleishman, Ruslan Korets, Peter Chang, Andrew Wagner, Boston, MA, Simon Kim, Aurora, CO, Joaquim Bellmunt, Irving Kaplan, Aria Olumi, Boris Gershman, Boston, MA
Introduction: Survival for patients with locally advanced bladder cancer following radical cystectomy (RC) remains poor. Although adjuvant chemotherapy (AC) is standard of care, one small randomized trial has suggested a potential disease-free survival benefit with the addition of post-operative radiotherapy (PORT). We therefore examined the association of PORT with overall survival (OS) in patients with locally advanced bladder cancer after RC.
Methods: Using a completed phase 2 trial to inform the design of the present study, we conducted observational analyses to emulate a hypothetical target trial of patients aged 18-79 years with pT3-4 Nany M0 or pTany N1-3 M0 urothelial carcinoma of the bladder following RC who were treated with AC (multiagent chemotherapy within 3 months of RC) with or without PORT (=45 Gy to the pelvis) from 2006-2015 in the National Cancer Database. Patients who received preoperative chemotherapy or radiotherapy were excluded. The associations of treatment arm with OS were evaluated using multivariable Cox regression.
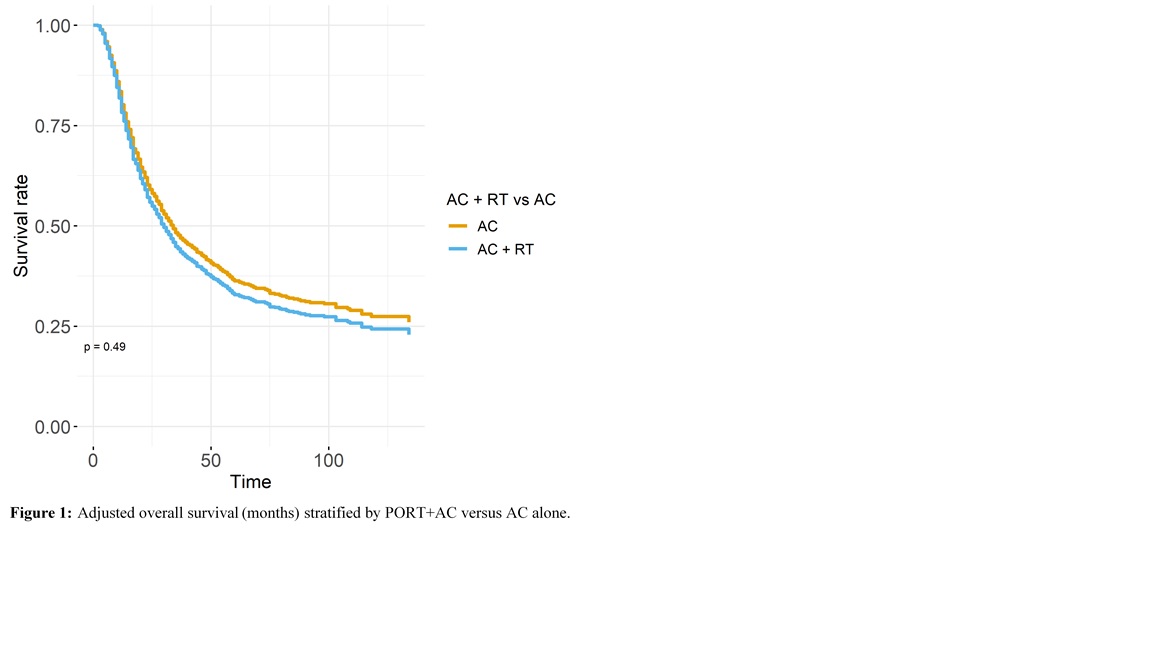
Results: A total of 1,684 patients were included, of whom 66 underwent PORT+AC and 1,618 AC alone. Compared to patients treated with AC alone, those treated with PORT+AC were more likely to have pT4 disease (52% vs 26%; p<0.01), have positive surgical margins (44% vs 17%; p<0.01), and be treated at a non-academic facility (75% vs 53%; p<0.01). Crude 3- and 5-year OS were 31% and 19% for PORT+AC versus 48% and 36% for AC alone (p=0.01). Adjusted 3- and 5-year OS were 44% and 33% for PORT+AC versus 48% and 36% for AC alone (p=0.49). After adjusting for baseline characteristics including pathologic features, PORT+AC was not associated with improved OS compared to AC alone (HR 1.11; 95% CI 0.82-1.51; Figure 1).
Conclusions: Although infrequently utilized, the present analyses suggest that the addition of radiotherapy to AC is not associated with improved OS in locally advanced bladder cancer. These results highlight the need for prospective trials to better define the potential benefits from PORT with regard to symptomatic progression and oncologic outcomes.

.jpg)
.jpg)