PD42-08: Real-World Performance of MRI After TURBT in Predicting Final Pathologic Outcomes in Bladder Cancer
Sunday, May 15, 2022
10:40 AM – 10:50 AM
Location: Room 245
Michael Chandra, Fort Worth, TX, Thomas Gerald*, Suzanne Cole, Liwei Jia, Jeffrey Howard, Dallas, TX, Aditya Bagrodia, San Diego, CA, Xiaosong Meng, Vitaly Margulis, Yair Lotan, Alberto Diaz de Leon, Solomon Woldu, Dallas, TX
Urologic Oncology Fellow University of Texas Southwestern Medical Center
Introduction: Bladder cancer staging by transurethral resection of a bladder tumor (TURBT) is often inaccurate due to limited sampling. For higher risk non-muscle invasive bladder cancer, the current standard is to repeat TURBT, an invasive procedure with associated risk and cost. Additionally, interest in bladder preservation following systemic therapy is limited by concerns regarding the accuracy of cystoscopic assessment of response. Bladder MRI has emerged as a potential non-invasive and accurate means of bladder cancer staging. We sought to examine the ability of MRI after TURBT to predict residual tumor and muscle-invasive bladder cancer (MIBC) in a real-world cohort of patients subsequently undergoing re-TURBT or cystectomy.
Methods: This prospectively maintained cohort evaluated 70 patients with bladder cancer who received a multiparametric pelvic MRI from 2019-2021 after TURBT. The MRI was protocoled for bladder cancer evaluation and included T2-, diffusion, and T1-weighed images with and without IV contrast. MRIs were evaluated for restricted diffusion, enhancement and signal intensity features indicative of residual tumor and MIBC. These results were then compared to final pathology at subsequent re-TURBT (n=42) or cystectomy (n=28).
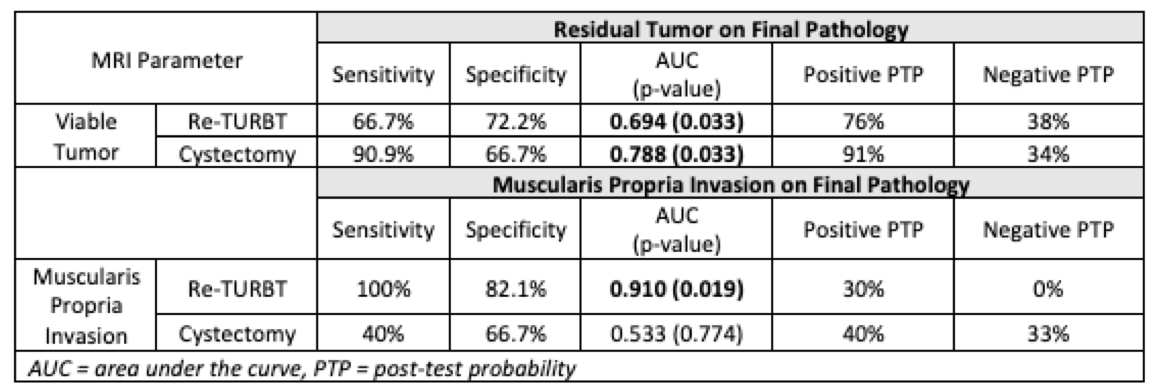
Results: Among re-TURBT cases, 24 (57.1%) and 3 (7.1%) had residual tumor and MIBC, respectively. Among cystectomy cases, 22 (78.6%) and 18 (64.3%) demonstrated residual tumor and MIBC, respectively. In detecting residual tumor among patients undergoing cystectomy, MRI showed a sensitivity, specificity, AUC, and positive post-test probability (PTP) of 90.9%, 66.7%, 0.788 (p=0.033), and 91%, respectively. In detecting MIBC among patients undergoing re-TURBT, MRI had a sensitivity, specificity, AUC, and negative PTP of 100%, 82.1%, 0.910 (p=0.019), and 0%, respectively.
Conclusions: In this real-world setting, MRI showed high performance in ruling out MIBC in patients undergoing re-TURBT and in predicting the presence of residual disease prior to cystectomy. Performance characteristics in other settings were less accurate. These findings support the continued refinement of MRI in bladder cancer and as a potentially important adjunct in specific scenarios.

.jpg)
.jpg)