Clinical Professor Nagasaki University School of Dentistry Saga Tosu, Japan
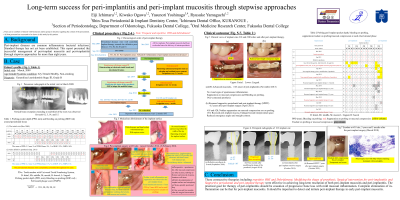
Background: Peri-implant diseases are common inflammatory bacterial infections. Standard therapy has not yet been established. This report presented the successful management of peri-implant mucositis and peri-implantitis through stepwise approaches for more than eight years.
Case: A 62-year-old, systemically healthy, non-smoker, Japanese woman with generalized periodontitis (stage Ⅲ, grade B) in March 2009. The patient’s periodontitis was well controlled with regular periodontal therapy. Implants were placed at #31, #30, #28, #20, and #18 tooth sites. Mucositis around all the implants were overlooked in March 2010. Peri-implantitis developed around #31, #30, and #18 implant sites. Clinical Procedures and Outcomes: Peri-implant mucositis was actively treated through non-surgical therapy and peri-implantitis through non-surgical therapy followed by additional surgical therapy, since November 2013, consecutively: OHIs, repetitive and meticulous nonsurgical debridement of implants, modification of prosthesis to improve oral hygiene, resective surgery through decontamination with implantoplasty, air-abrasion using β-TCP powder, and a mesio-apically positioned flap; supportive peri-implant therapy with repetitive debridement of the implant surfaces every one to two months. The peri-implant inflammation and bone resorption resolved seven years after the surgical therapy. A small amount of exudate dominant with neutrophils was occasionally observed at the #18 implant site.
Conclusion: These consecutive therapies were effective in achieving long-term resolution of both peri-implant mucositis and peri-implantitis. The practical goal for therapy of peri-implantitis should be cessation of progressive bone loss with mild mucosal inflammation. Complete elimination of inflammation can be that for peri-implant mucositis. It should be important to detect and initiate peri-implant therapy in early peri-implant mucositis.

 photo")