
Poster Session D
Crystal arthropathies
Gary Ho, MD
NYU Langone Health
Brooklyn, NY, United States
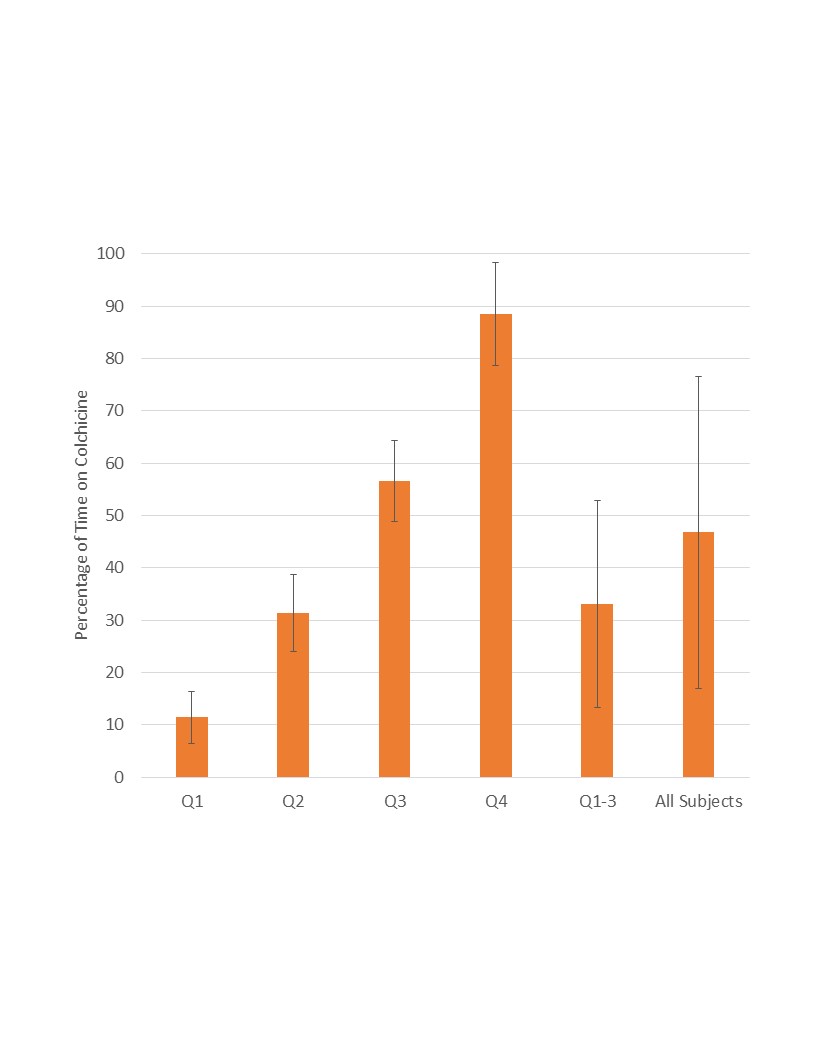 Mean and standard deviation percentage of time on colchicine within each quartile, Quartiles 1-3, and all subjects.
Mean and standard deviation percentage of time on colchicine within each quartile, Quartiles 1-3, and all subjects..jpg) Incidence of first MACE and sub-component events in Quartiles 1-3 versus Quartile 4.
Incidence of first MACE and sub-component events in Quartiles 1-3 versus Quartile 4..jpg) Kaplan-Meier survival curves in Quartiles 1-3 and Quartile 4 illustrating the cumulative proportion of patients experiencing a first MACE over time; maximum observation period of 10 years. Patients censored at the end of their respective observation periods are demarcated by a vertical line.
Kaplan-Meier survival curves in Quartiles 1-3 and Quartile 4 illustrating the cumulative proportion of patients experiencing a first MACE over time; maximum observation period of 10 years. Patients censored at the end of their respective observation periods are demarcated by a vertical line.