Poster Session C
Epidemiology, health policy and outcomes
Jo Anne Marcuz, PT
The Hospital for Sick Children
Toronto, ON, Canada
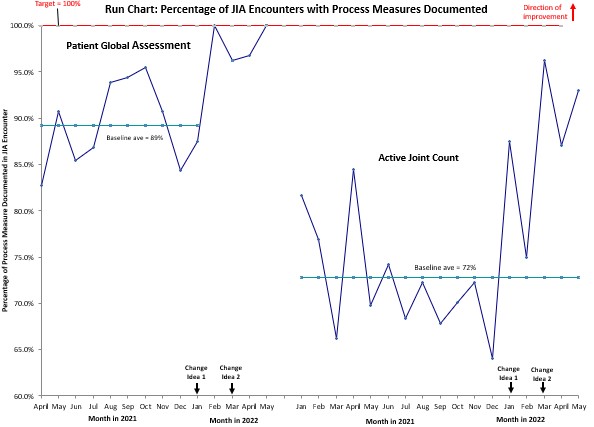
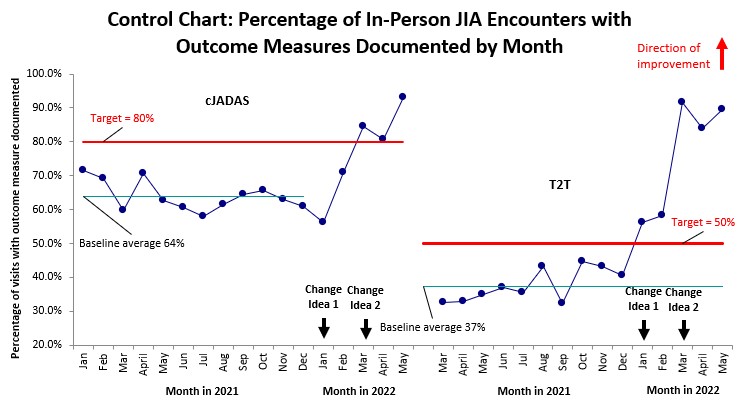
.jpg) PGA = physician global assessment; PtGA = patient global assessment; AJC = active joint count; cJADAS = clinical juvenile arthritis disease activity score; T2T = treat to target (specifically “new target” documented).
PGA = physician global assessment; PtGA = patient global assessment; AJC = active joint count; cJADAS = clinical juvenile arthritis disease activity score; T2T = treat to target (specifically “new target” documented).