Abstract Session
.png "Mary-Ann Fitzcharles, MD, FRCPC photo")
Mary-Ann Fitzcharles, MD, FRCPC
McGill University
Montreal-West, QC, Canada
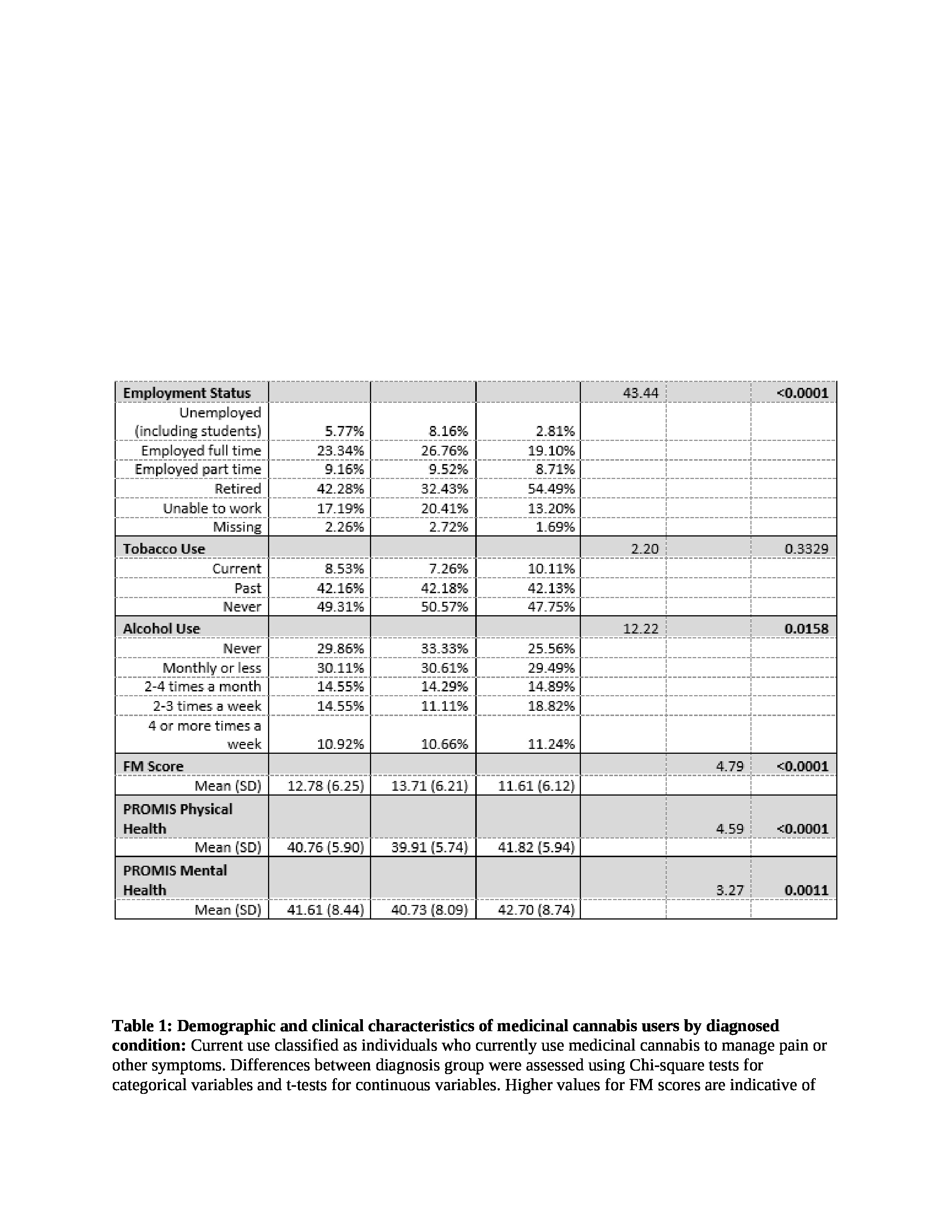 Table 1: Demographic and clinical characteristics of medicinal cannabis users by diagnosed condition: Current use classified as individuals who currently use medicinal cannabis to manage pain or other symptoms. Differences between diagnosis group were assessed using Chi-square tests for categorical variables and t-tests for continuous variables. Higher values for FM scores are indicative of more severe fibromyalgia symptoms, whereas higher PROMIS scores demonstrate greater physical and mental health.
Table 1: Demographic and clinical characteristics of medicinal cannabis users by diagnosed condition: Current use classified as individuals who currently use medicinal cannabis to manage pain or other symptoms. Differences between diagnosis group were assessed using Chi-square tests for categorical variables and t-tests for continuous variables. Higher values for FM scores are indicative of more severe fibromyalgia symptoms, whereas higher PROMIS scores demonstrate greater physical and mental health.