
Abstract Session
Epidemiology, health policy and outcomes
Jason Jakiela, MS
University of Delaware
Newark, DE, United States
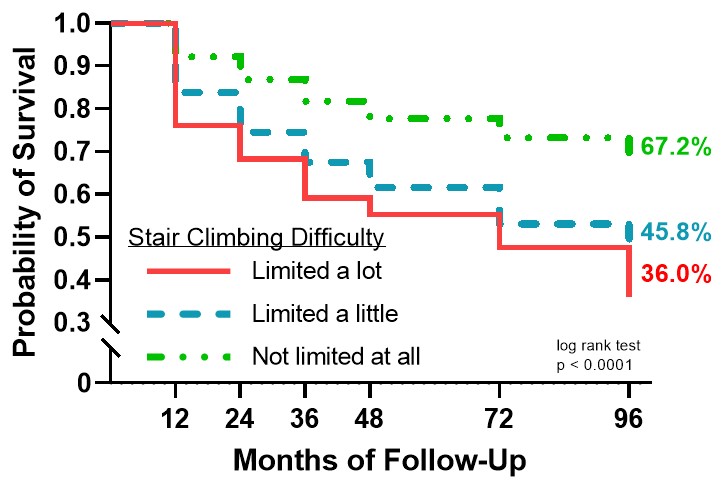 Figure 1: Kaplan-Meier survival curve for walking speed functional limitation by stair climbing difficulty group
Figure 1: Kaplan-Meier survival curve for walking speed functional limitation by stair climbing difficulty group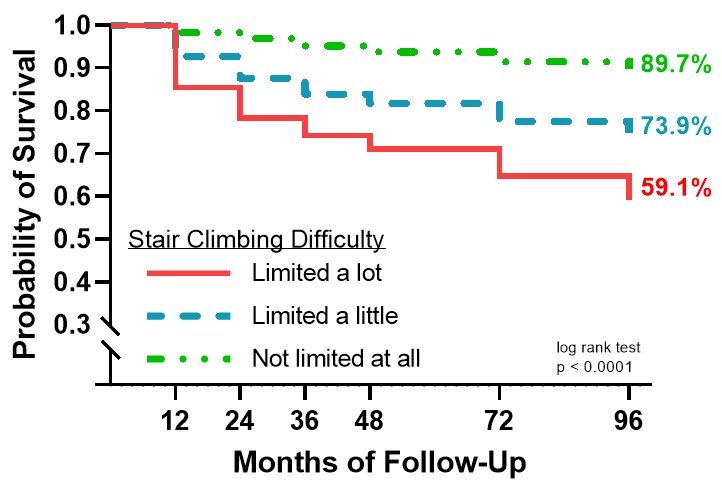 Figure 2: Kaplan-Meier survival curve for WOMAC-PF functional limitation by stair climbing difficulty group
Figure 2: Kaplan-Meier survival curve for WOMAC-PF functional limitation by stair climbing difficulty group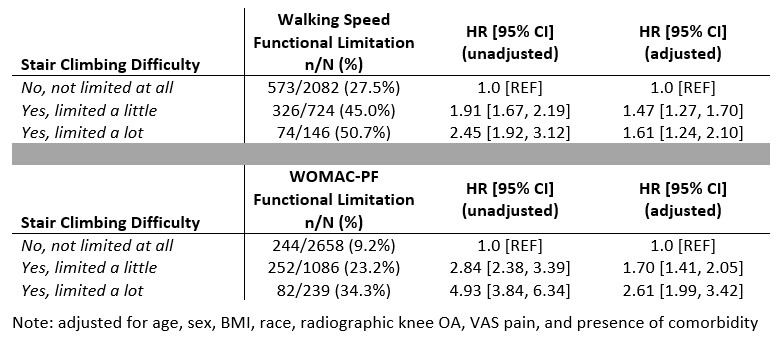 Table 1: Hazard ratios (HRs) & 95% confidence intervals (95% CIs) for walking speed and WOMAC-PF functional limitation by stair climbing difficulty group
Table 1: Hazard ratios (HRs) & 95% confidence intervals (95% CIs) for walking speed and WOMAC-PF functional limitation by stair climbing difficulty group