
Poster Session D

Tala El Tal, MD
University of Toronto/Hospital for Sick Children
Toronto, ON, Canada
.jpg) Table 1: cSLE Demographics, Disease Characteristics, and Patient-Reported Outcomes
Table 1: cSLE Demographics, Disease Characteristics, and Patient-Reported Outcomes .jpg) Table 2: Spearmen correlations between Global Executive Composite (GEC) T scores and disease-related factors, and PROMIS measures.
Table 2: Spearmen correlations between Global Executive Composite (GEC) T scores and disease-related factors, and PROMIS measures. 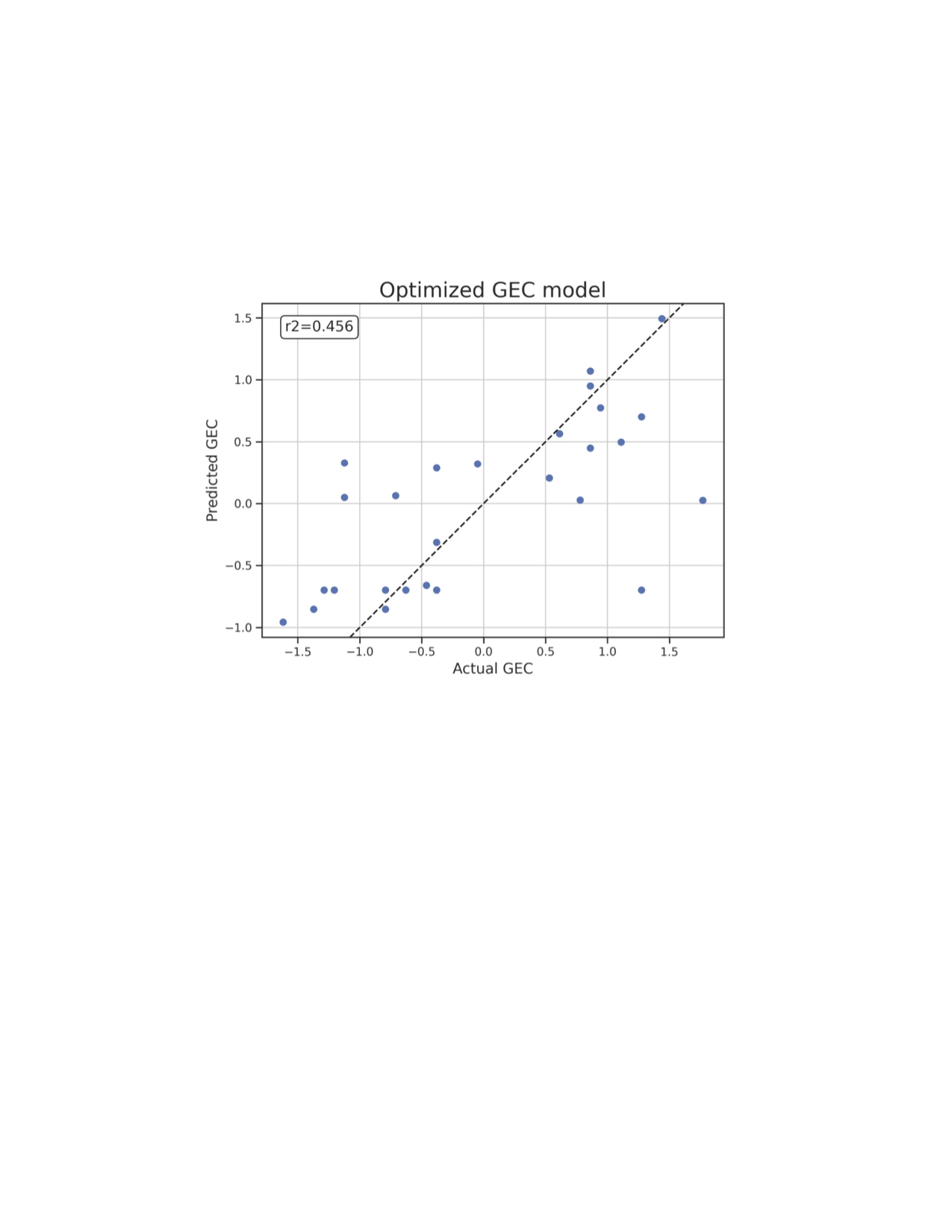 Partial Least Square (PLS2) regression analysis enables description of interactions between multivariate and potentially collinear data with a relatively small sample size. Each predictor’s relevance criterium was based on the bootstrapped sample distribution of its variable importance in projection (VIP) value (significant if VIP > 1, CI = 95%). Relevant predictors for this model include SDI (coeff =0.58), pain behavior (coeff=0.41), and steroid use at visit (coeff=-0.38) and pain interference (coeff=0.35) ranked based on coefficients (coeff). Increased SDI and pain but less steroid use at visit predicts worse GEC scores.
Partial Least Square (PLS2) regression analysis enables description of interactions between multivariate and potentially collinear data with a relatively small sample size. Each predictor’s relevance criterium was based on the bootstrapped sample distribution of its variable importance in projection (VIP) value (significant if VIP > 1, CI = 95%). Relevant predictors for this model include SDI (coeff =0.58), pain behavior (coeff=0.41), and steroid use at visit (coeff=-0.38) and pain interference (coeff=0.35) ranked based on coefficients (coeff). Increased SDI and pain but less steroid use at visit predicts worse GEC scores. 