
Ignite Talk

Cecilia Chung, MD, MPH
Vanderbilt University Medical Center
Nashville, TN, United States
Disclosure: Disclosure information not submitted.
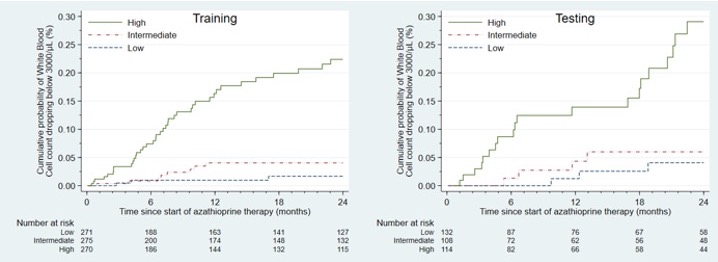 Association between a score combining genetic and clinical data and cumulative incidence of leukopenia
Association between a score combining genetic and clinical data and cumulative incidence of leukopenia