
Poster Session B
Epidemiology, health policy and outcomes
Eugene Looi, MD
Loma Linda University
Loma Linda, CA, United States
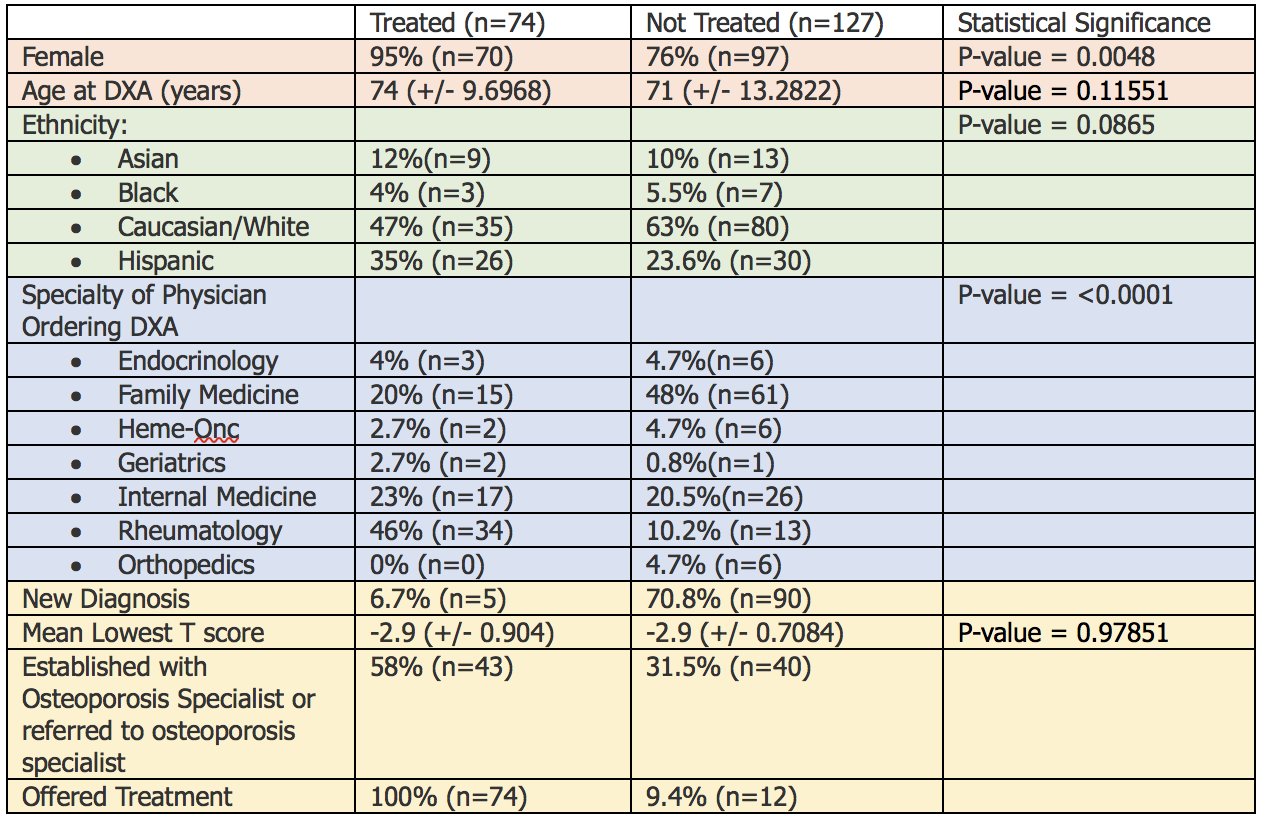 Table 1: Comparison of Treated vs. Not Treated Osteoporosis Patients
Table 1: Comparison of Treated vs. Not Treated Osteoporosis Patients 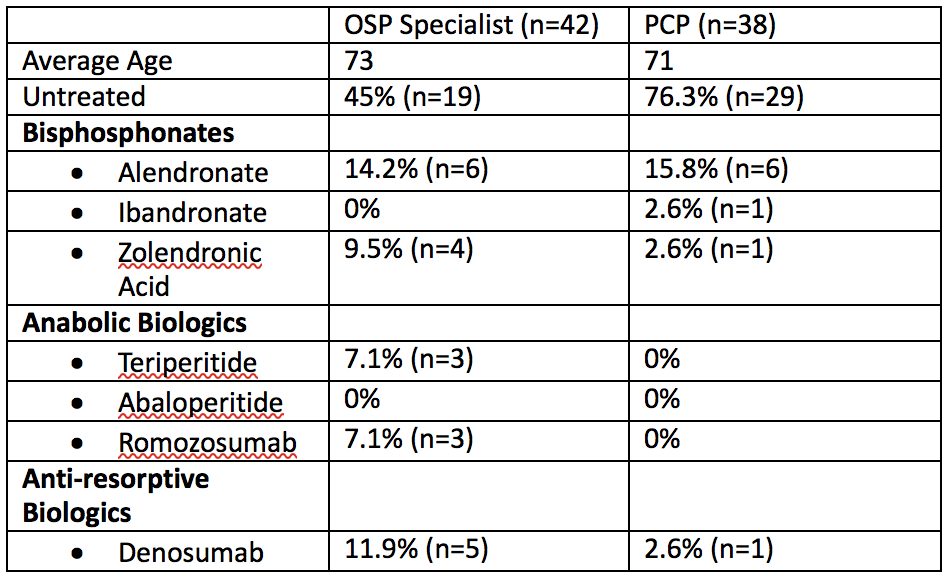 Table 2: High Risk Osteoporosis Patients (T-score ≤ -3.0)
Table 2: High Risk Osteoporosis Patients (T-score ≤ -3.0) 