
Abstract Session
Walter P. Maksymowych, MD
University of Alberta
Edmonton, AB, Canada
.jpg) Table 1. Frequency of Spinal MRI lesions According to an MRI SIJ scan Positive for AxSpA
Table 1. Frequency of Spinal MRI lesions According to an MRI SIJ scan Positive for AxSpA 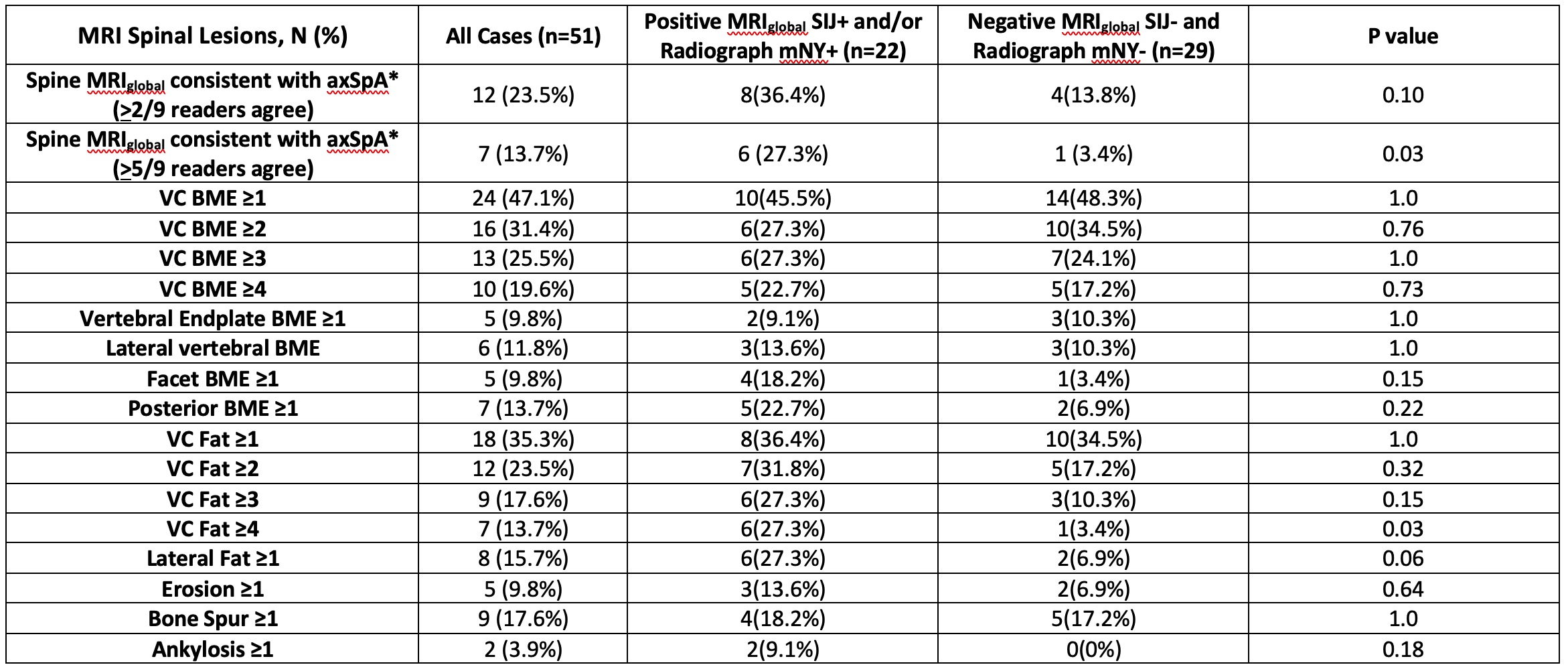 Table 2. Frequency of Spinal MRI lesions According to an MRI SIJ scan Positive for AxSpA and/or Presence/Absence of Radiographic Sacroiliitis (mNY+)
Table 2. Frequency of Spinal MRI lesions According to an MRI SIJ scan Positive for AxSpA and/or Presence/Absence of Radiographic Sacroiliitis (mNY+)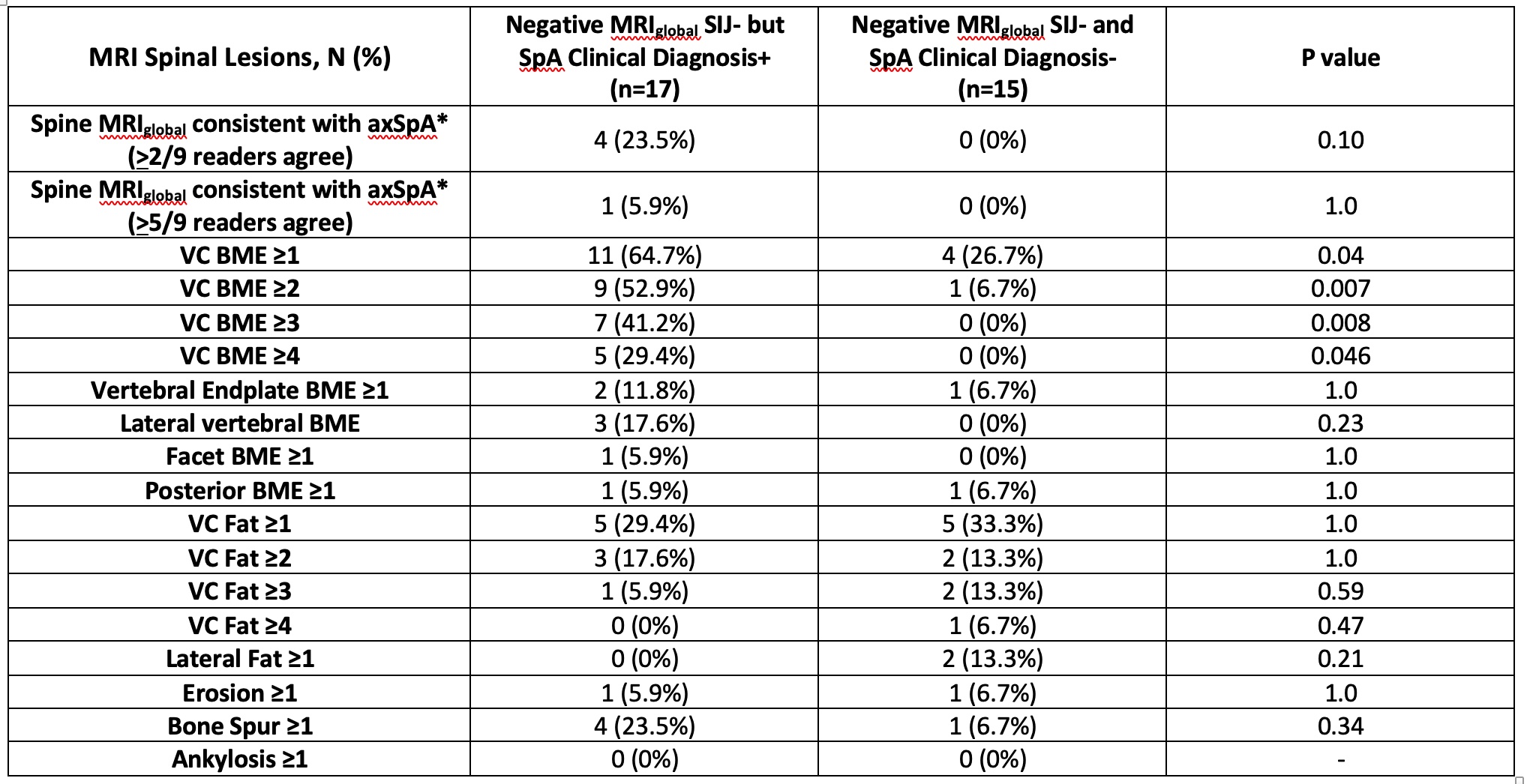 Table 3. Frequency of Spinal MRI lesions in Cases with Negative MRI SIJ scan for AxSpA according to Presence/Absence of Clinical Diagnosis of axSpA
Table 3. Frequency of Spinal MRI lesions in Cases with Negative MRI SIJ scan for AxSpA according to Presence/Absence of Clinical Diagnosis of axSpA