
Poster Session C
Epidemiology, health policy and outcomes
Sho Fukui, MD, MPH
Kyorin University Hospital
Tokyo, Japan
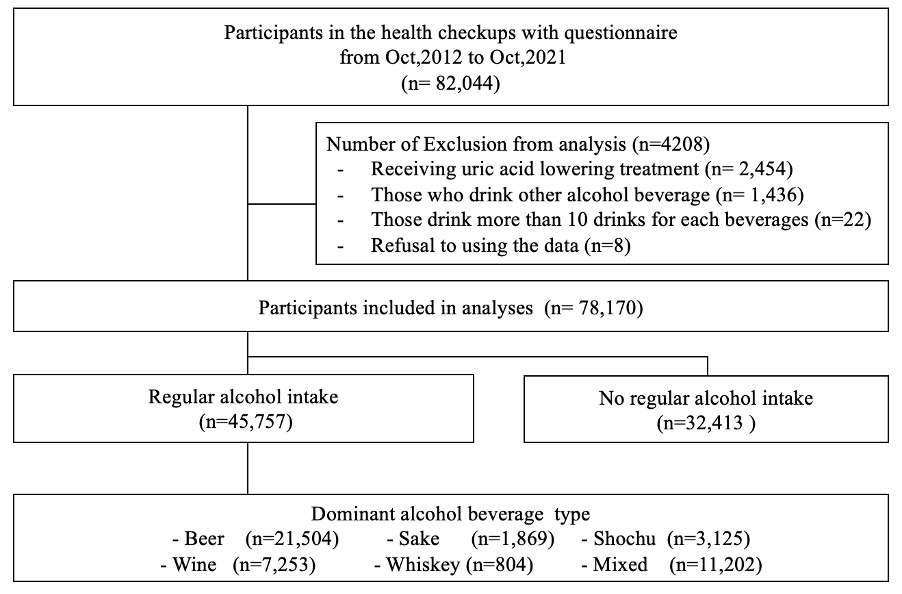 Figure 1. Flow chart of inclusion and exclusion of participants
Figure 1. Flow chart of inclusion and exclusion of participants.jpg) Figure 2 Types of Dominant Alcohol Beverages and Predicted serum urate
Figure 2 Types of Dominant Alcohol Beverages and Predicted serum urate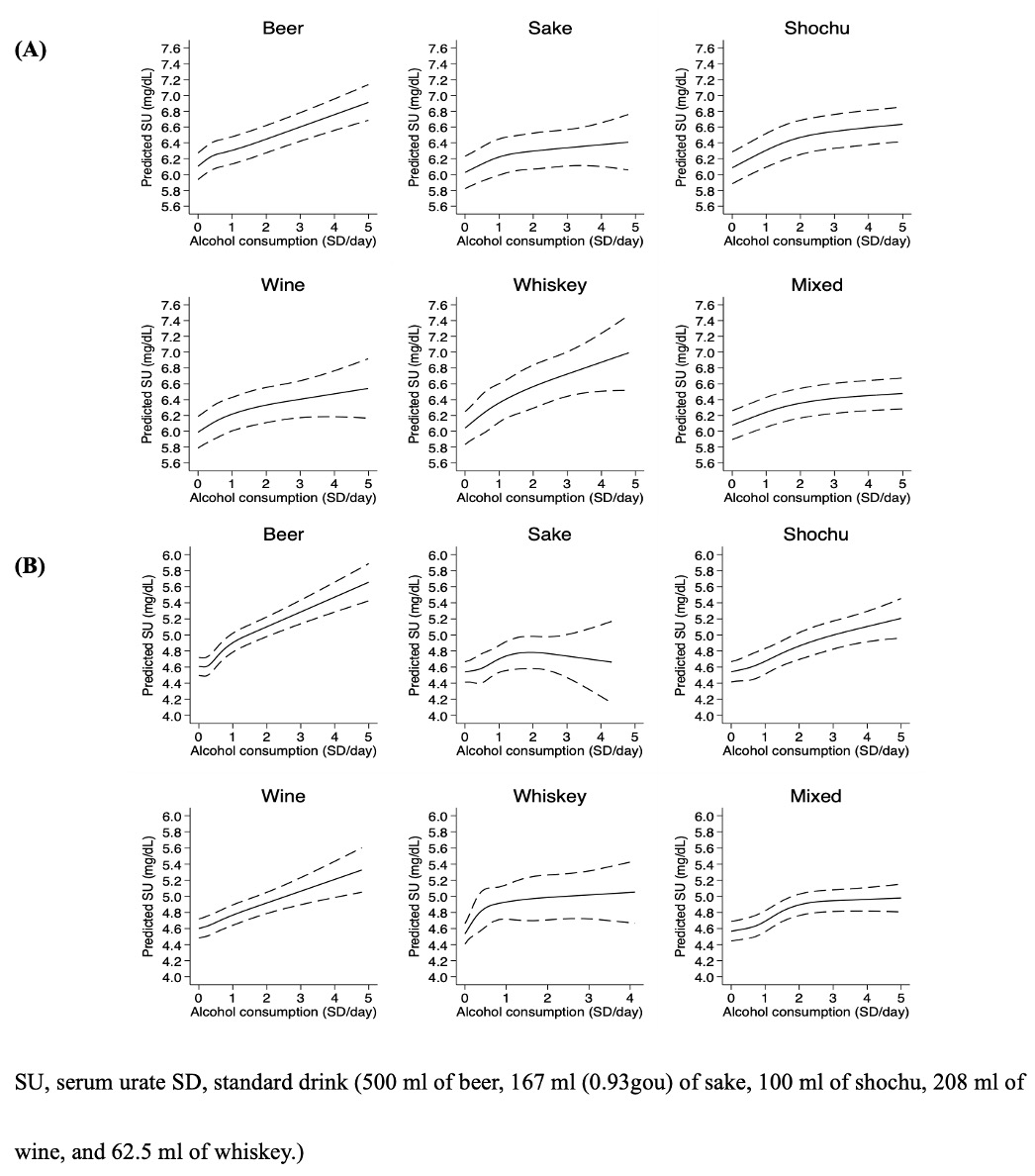 Figure 3. Predicted serum urate and alcohol consumption in each dominant alcohol beverage type using restricted cubic spline with knots by percentile (5, 35, 65, 95) in (A) Male and (B) Female.
Figure 3. Predicted serum urate and alcohol consumption in each dominant alcohol beverage type using restricted cubic spline with knots by percentile (5, 35, 65, 95) in (A) Male and (B) Female.