Kenneth Chow, MD, Steve Hu, MD, Cameron Sikavi, MD, Matthew Bell, MD, Brandon Gisi, MD, Viktor Eysselein, MD, Sofiya Reicher, MD Harbor-UCLA Medical Center, Torrance, CA
Introduction: Pancreatic ductal adenocarcinoma (PDAC) classically presents as a solitary pancreatic mass on cross-sectional imaging. Diffuse-type PDAC (DTP) is an unusual variant that accounts for 1-5% of PDAC. Due to its rarity, there are no established radiographic or endoscopic definitions of DTP. Previous case reports describe presentations of DTP either as a solitary pancreatic mass or diffuse pancreatic enlargement. We report a unique case of DTP presenting with CT findings of two distinct masses in the pancreatic head and tail, and with EUS findings of diffuse gland enlargement mimicking autoimmune pancreatitis.
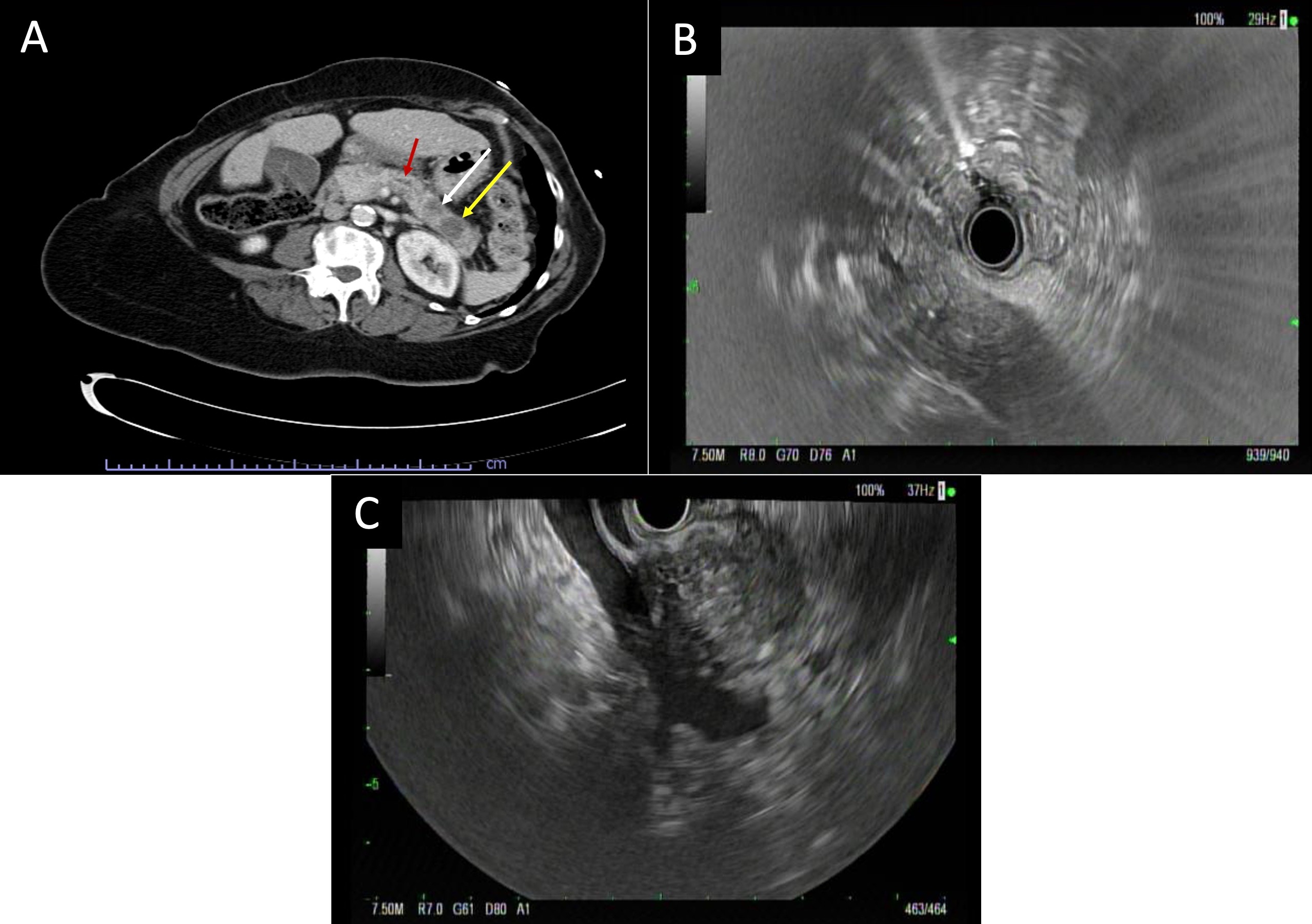
Case Description/Methods: A 70-year-old female presented with two weeks of severe epigastric pain and unintentional weight loss. A CT scan showed two distinct pancreatic masses measuring 2.3 x 1.6 cm and 1.6 x 1.0 cm in the head and tail respectively (Figure 1A). EUS demonstrated a “sausage-shaped” diffusely enlarged pancreas with duct dilation of 2.5 mm in the body; no discrete lesions were seen (Figure 1B, 1C). Workup for autoimmune pancreatitis was negative with normal IGG4 levels. EUS-FNB of the pancreatic head revealed infiltrating adenocarcinoma. A repeat CT scan showed interval enlargement of the tail mass and subsequent EUS-FNB of the pancreas tail returned with moderately differentiated invasive adenocarcinoma. ERCP performed for worsened liver function tests demonstrated a 3 cm stricture of the distal common bile duct, which was managed with a fully-covered metal stent. A multi-disciplinary tumor board deemed the neoplasm borderline-resectable diffuse-type PDAC, and the patient was started on a neoadjuvant chemotherapy regimen of gemcitabine and abraxane in preparation for total pancreatectomy.
Discussion: The differential for multiple pancreatic masses is broad and includes autoimmune pancreatitis, secondary metastases, and pancreatic neuroendocrine neoplasms. DTP is a rare manifestation of PDAC and little is known about its etiology and endoscopic findings. DTP could stem from progression of a focal PDAC or could result from synchronous multifocal tumor development. To our knowledge, this is the first documented case of DTP presenting with multiple pancreatic masses and EUS findings mimicking autoimmune pancreatitis. The case illustrates the importance of sampling several areas of the pancreas when diffuse enlargement is present on EUS and multiple pancreatic masses are seen on cross-sectional imaging.
Figure: Figure 1. A. Axial-oblique CT demonstrates a low-density lesion in the pancreatic tail (yellow arrow) measuring 2.3 x 1.6 cm. An adjacent ill-defined low-density lesion (white arrow) measures 1.6 x 1.0 cm. The pancreas is borderline in size and the pancreatic duct is prominent (red arrow). B. EUS demonstrates a diffusely enlarged pancreas with the head, body, and tail displaying a diffusely hypoechoic “sausage-like” appearance. C. EUS demonstrates focal prominence of the pancreatic head with loss of interface with the portal vein-superior mesenteric vein confluence.
Disclosures:
Kenneth Chow indicated no relevant financial relationships.
Steve Hu indicated no relevant financial relationships.
Cameron Sikavi indicated no relevant financial relationships.
Matthew Bell indicated no relevant financial relationships.
Brandon Gisi indicated no relevant financial relationships.
Viktor Eysselein indicated no relevant financial relationships.
Sofiya Reicher indicated no relevant financial relationships.
Kenneth Chow, MD, Steve Hu, MD, Cameron Sikavi, MD, Matthew Bell, MD, Brandon Gisi, MD, Viktor Eysselein, MD, Sofiya Reicher, MD. C0049 - Diffuse-Type Pancreatic Ductal Adenocarcinoma Mimicking Autoimmune Pancreatitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.