Introduction: Eosinophilic gastrointestinal disorders (EGIDs) refer to eosinophilic infiltration of the gastrointestinal tract in the absence of secondary causes. Here, we present a case of a young male with immune thrombocytopenia (ITP) and biopsy-proven eosinophilic gastroenteritis that developed iron-deficiency anemia.
Case Description/Methods: A 16-year old male with a past medical history significant for autism, ITP, melanoma, allergic rhinitis, and eosinophilic esophagitis presented for evaluation of chronic abdominal pain.
He had an EGD in April 2018 that revealed white exudates at the gastroesophageal junction, scattered erosions in the gastric body and fundus, severe antral gastritis, and scattered erosions noted throughout the duodenal bulb. Biopsies were taken and revealed distal eosinophilic esophagitis (greater than 50/HPF), eosinophilic gastritis, and chronic inflammation of the duodenal bulb with Brunner gland hyperplasia and villous blunting. Absolute eosinophil count was higher than 2,000/uL. Given findings of persistent inflammation despite a six-food elimination diet, the patient was started on oral Budesonide, a proton-pump inhibitor, and an H2 receptor blocker.
In March 2020, a repeat surveillance EGD with biopsy revealed the duodenum was free of inflammation or other diagnostic abnormalities. Roughly 28 eosinophils/HPF were present in the gastric cardia near the GEJ, and numerous eosinophils remained in the other gastric tissues sampled. Budesonide was discontinued due to patient intolerance.
In early 2021, the patient was found to have microcytic anemia. Further Hematologic evaluation revealed low folate and iron levels. He was started on supplemental iron and folic acid, leading to resolution of the anemia. Iron and folate deficiency was believed to be secondary to malabsorption caused by EGE.
Discussion: Eosinophilic gastrointestinal diseases remain a rare and underexplored clinical entity. While its pathophysiology is not fully understood at this time, TH2 mediated activation of B-cells and subsequent stimulation of eosinophils locally appears to be at play. Given ITP has a TH1 predominant cytokine profile, it is unclear if there is a causal association between the two. Diagnosis of EGID necessitates histological evidence of eosinophilic infiltration of the GI tract in the absence of secondary causes or infiltration elsewhere. Dietary modification to eliminate food allergens is a reasonable initial treatment, glucocorticoids remain the mainstay of pharmacotherapy at this time.
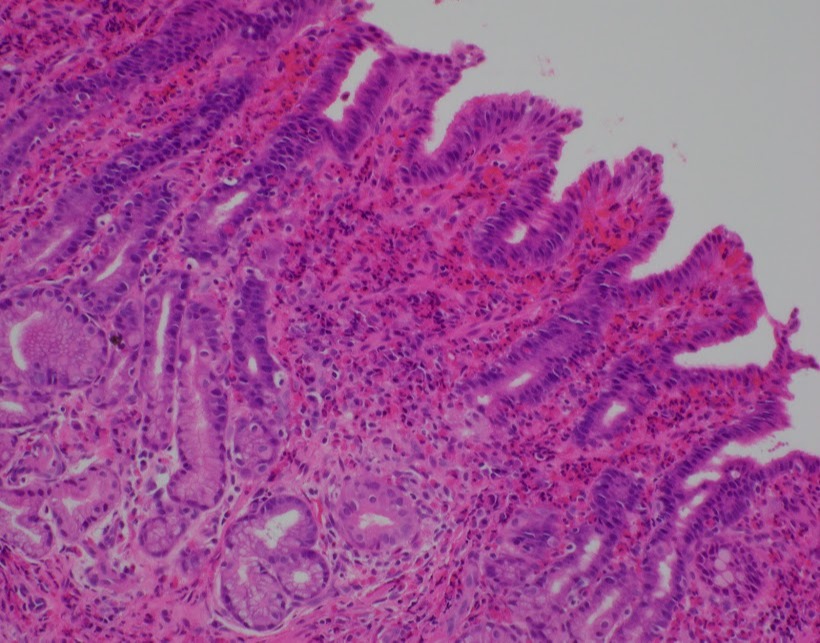
Figure: Figure 1: Cross-section of gastric tissue stained with hematoxylin and eosin demonstrating prominent eosinophils (greater than 100 per high-power field) within the lamina propria and gastric epithelium with associated epithelial injury.
Disclosures:
Gurdeep Singh indicated no relevant financial relationships.
Aimen Farooq indicated no relevant financial relationships.
Baha Aldeen Bani Fawwaz indicated no relevant financial relationships.
Arooj Mian indicated no relevant financial relationships.
Abu Hurairah indicated no relevant financial relationships.
Gurdeep Singh, DO, Aimen Farooq, MD, Baha Aldeen Bani Fawwaz, MBBS, Arooj Mian, MD, Abu Hurairah, MD. B0699 - March of the Eosinophils: A Case of Eosinophilic Gastroenteritis, Immune Thrombocytopenia, and Iron Deficiency Anemia, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.