Emily Smith, MD1, Jose Jessurun, MD2, Dana Lukin, MD, PhD1, Paris Charilaou, MD1 1Weill Cornell Medicine, New York, NY; 2NewYork Presbyterian-Weill Cornell Medical Center, New York, NY
Introduction: Protein losing enteropathy (PLE) can be classified into erosive, non-erosive, and increased interstitial pressure PLE. Presenting signs are often chronic non-bloody diarrhea, anasarca, abdominal pain, and weight loss. We present a complex case of a PLE presentation with a novel diagnosis.
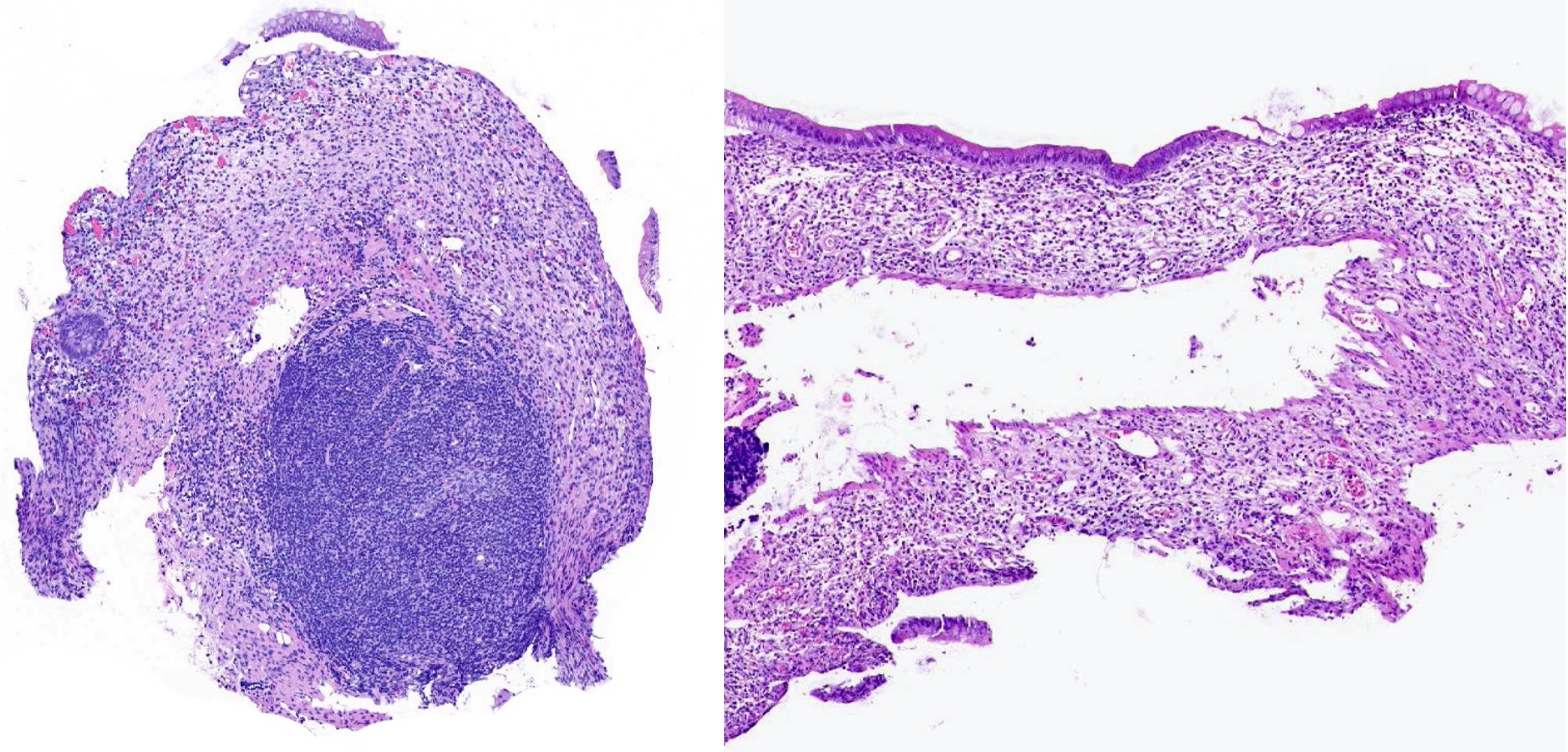
Case Description/Methods: A 30-year-old woman with a history of migraines presented with severe abdominal pain and chronic diarrhea. She was on long-term combined estrogen-progestin oral contraceptive pills (OCP) and chronic high dose non-steroidal anti-inflammatory (NSAID) medications. She was exposed to mycoplasma pneumoniae one month prior to presentation, without other infectious exposures. Laboratory tests were notable for hemoglobin 6 g/dL, albumin 0.5 g/dL, stool pathogen PCR negative, and fecal calprotectin >3000µg/g. Extensive infectious work up only revealed Mycoplasma IgM+. Inflammatory markers and alpha-1 anti-trypsin clearance were elevated, and she was found to have warm autoimmune hemolytic anemia. CT angiography excluded ischemia and vasculitis (autoimmune serologies were negative), revealing diffuse enterocolitis, confirmed on magnetic resonance enterography with ileal ulcers. Endoscopic evaluation revealed diffuse superficial ulcerations terminal ileum and colon with diffuse mucosal sloughing. Histopathology revealed diffusely injured crypts with crypt drop-out and minimal inflammation, without any findings to suggest infection, inflammatory bowel disease (IBD) or autoimmune enteritis (Figure 1). Normal B-cell switching studies excluded common variable immunodeficiency (CVID). Due to profound anasarca and inability to tolerate oral intake, albumin infusions and total parenteral nutrition were started. There was minimal response to systemic or topical steroids. Diarrhea was mildly improved with albumin repletion, and she was empirically started on vedolizumab.
Discussion: Given the absence of classic IBD findings, negative infectious and immunological testing, we present the first case of autoimmune cryptolytic enterocolitis, a histopathologic diagnosis of unclear etiology and pathogenesis. The patient has responded to vedolizumab infusions as an empiric treatment for an IBD-like entity. Nevertheless, supporting the autoimmune component of this entity, is a possible concomitant potential pathway of molecular mimicry in the setting of post-mycoplasma infection along with chronic high dose NSAID and OCP exposure.
Figure: Terminal Ileum and Sigmoid Colon with Diffuse Crypt Dropout
Disclosures:
Emily Smith indicated no relevant financial relationships.
Jose Jessurun indicated no relevant financial relationships.
Paris Charilaou indicated no relevant financial relationships.
Emily Smith, MD1, Jose Jessurun, MD2, Dana Lukin, MD, PhD1, Paris Charilaou, MD1. B0428 - A New Protein Losing Enteropathy: Autoimmune Cryptolytic Enterocolitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.