Atrium Health Wake Forest Baptist Winston-Salem, NC
Ted G. Xiao, MS, MD1, Nicholas J. Koutlas, MD2, Rishi Pawa, MBBS1 1Atrium Health Wake Forest Baptist, Winston-Salem, NC; 2Atrium Health - Wake Forest Baptist, Winston-Salem, NC
Introduction: A biloma is a well-defined collection of bile outside the biliary tree typically caused by iatrogenic disruption of a bile duct. Percutaneous drainage is the traditional treatment modality with surgery reserved for refractory cases. Endoscopic ultrasound (EUS) guided transenteric drainage has emerged as a suitable alternative. We present a case of an infected post-cholecystectomy biloma treated using EUS-guided drainage with a transgastric LAMS.
Case Description/Methods: A 57-year-old female presented with fevers, abdominal pain, nausea, and vomiting following a laparoscopic cholecystectomy for acute cholecystitis 12 days prior. Labs noted a leukocytosis with normal liver chemistries. CT scan of the abdomen showed a peripherally enhancing gas and fluid collection in the subhepatic space measuring 14.5 x 7 x 8 cm, resulting in a mass effect on the antrum and proximal duodenum. Gastroenterology was consulted for the management of suspected bile leak and infected biloma.
Endoscopic retrograde cholangiography (ERC) revealed a bile leak with contrast extravasation from the cystic duct stump. This was treated with biliary sphincterotomy and placement of a 10 Fr x 7 cm plastic biliary stent. Same session EUS demonstrated a large fluid collection abutting the antrum with a well-defined wall. EUS-guided drainage of the biloma was performed using a 15 x 10 mm electrocautery enhanced LAMS via a transgastric approach. Approximately 1 L of purulent fluid was evacuated from the cavity. A subsequent CT scan confirmed the correct positioning of the LAMS with marked cavity decompression. The patient’s symptoms resolved.
Endoscopy with LAMS removal and placement of 2 10 Fr x 4 cm double pigtail stents (DPT) was performed 1 week later. CT 1 week after DPT placement noted near-complete resolution of the fluid collection. Six weeks after the index procedure, ERC showed resolution of the cystic duct leak and the biliary stent was removed. Both DPTs were removed 2 weeks later. The patient has remained well clinically.
Discussion: EUS-guided transenteric biloma drainage is a safe and effective alternative to percutaneous drainage. Initial cases were performed using plastic stents but more recently, transduodenal drainage with a LAMS was reported. Endoscopic drainage also enables same session identification and treatment of the culprit bile leak which is essential to prevent biloma recurrence. Our case is the first reported EUS-guided transgastric drainage of an infected biloma using a LAMS.
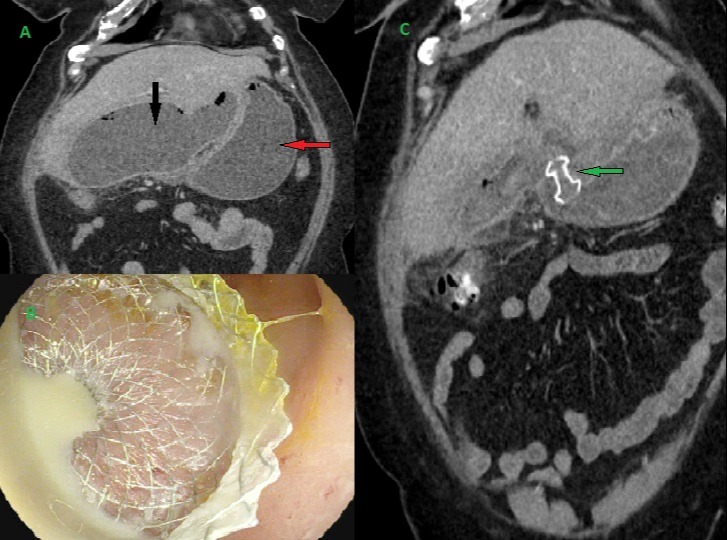
Figure: Figure 1. A. CT scan illustrating a large subhepatic fluid and gas-containing collection (black arrow) with resultant gastric outlet obstruction (red arrow). B. Successful placement of a transgastric lumen apposing metal stent (LAMS) into the biloma cavity with immediate drainage of purulent fluid. C. Post-drainage CT scan demonstrating biloma cavity decompression and appropriate positioning of the LAMS (green arrow).
Disclosures:
Ted Xiao indicated no relevant financial relationships.
Nicholas Koutlas indicated no relevant financial relationships.
Rishi Pawa indicated no relevant financial relationships.
Ted G. Xiao, MS, MD1, Nicholas J. Koutlas, MD2, Rishi Pawa, MBBS1. E0066 - Endoscopic Ultrasound-Guided Transgastric Drainage of an Infected Biloma After Cholecystectomy: A Case Report, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.