Pujan Kandel, MD1, Deepa Wosti, MBBS2, Murtaza Hussain, MD3, Dipesh Rohita, MBBS4, Frank Lukens, MD1, Bhaumik Brahmbhatt, MD1 1Mayo Clinic Jacksonville, Jacksonville, FL; 2Chitwan Medical College, Kathmandu, Bagmati, Nepal; 3Hurley Medical Center at Michigan State University, Flint, MI; 4B.P. Koirala Institute of Health Sciences, Jankpurdham, Janakpur, Nepal
Introduction: Majority of the color cancer rise from benign colorectal polyps. Endoscopic management now a days is a standard method of treatment is associated with lower mortality, morbidities, and cost. Despite good evidence of endoscopic treatment of colorectal polyps, surgical resection/colectomy is routinely performed in United States. The main objective of this study is to evaluate the predictors of in-hospital mortality and hospital length of stay after surgery of nonmalignant colorectal polyps.
Methods: We analyzed the data between January 1, 2012, and December 31, 2019, from the National Inpatient Sample (NIS) database. Discharged adult patients (≥18 years old) hospitalized for non-malignant colonic or anorectal polyp as principal diagnosis and who underwent colectomy or proctectomy as a primary procedure were included. The principal or primary diagnosis is the unique diagnosis during the hospitalization for which the patient was primarily admitted or treated. Patients with any diagnosis of colorectal cancer using both the ICD 9, ICD 10 diagnosis, and procedural codes were excluded from our analysis.
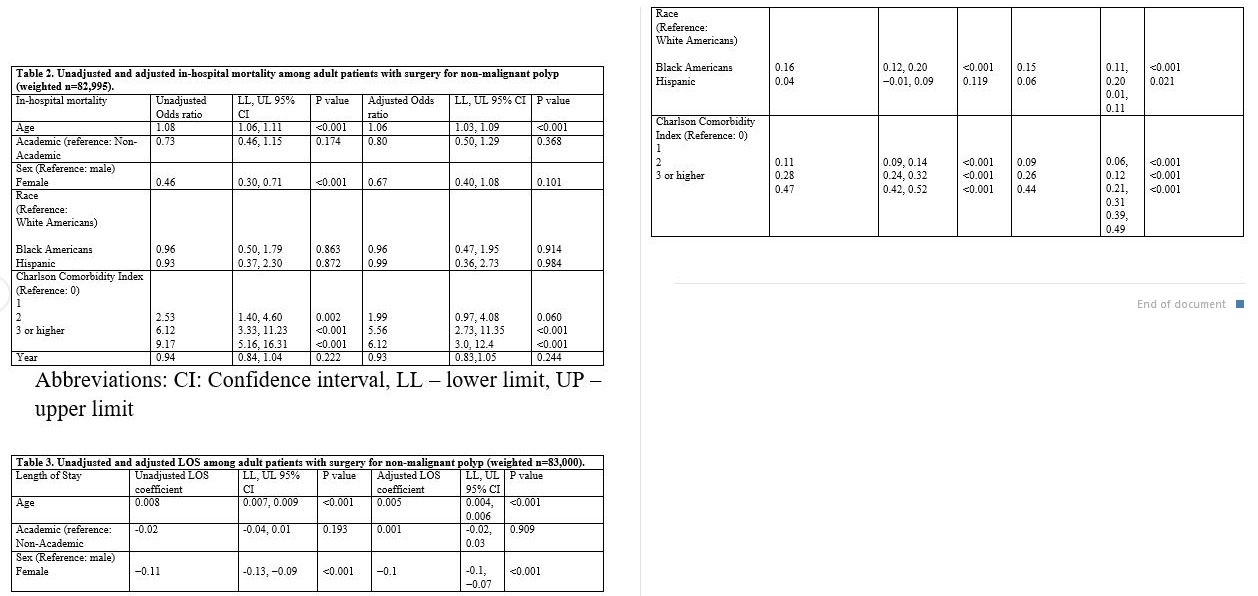
Results: There were 99330 primary admissions for surgical resection of non-malignant polyp resection in the United States from the year 2012 to 2019. Fifty one percent cases were female (n=50191) and 66 % cases (n=59407) from academic hospitals. Unadjusted univariate regression models demonstrated-age, sex, and higher comorbidity category were associated with increase in-hospital mortality. Also, hospitalizations with CCI (Charlson-comorbidity-index) of 2 (adjusted odds ratio, aOR 5.56; 95% CI: 2.73, 11.35; p< 0.001) or higher [CCI 3 and above] (aOR 6.12; 95% CI: 3, 12.4; p< 0.001) had a statistically significant higher likelihood of in-hospital mortality than those in the lower morbidity category. Females had significantly lower LOS after adjusting for covariates (age, hospital teaching status, race, CCI, and year) [adjusted coefficient (β)= -0.1; 95% CI: -0.1, -0.07, p< 0.001]. No significant difference was found in LOS and in-hospital mortality between academic and non-academic hospitals- [adjusted coefficient (β)= 0.001; 95% CI: -0.02, 0.03, p=909] and (adjusted odds ratio, aOR 0.80; 95% CI: 0.50, 1.29; p=0.368)
Discussion: Surgery with higher comorbidities is associated with increase in-hospital mortality. There endoscopic management of colorectal polyps should be highly considered. Appropriate selection of patient is important for best possible outcome.
Figure: Adjusted/unadjusted in-hospital mortality and length of stay
Table: NA
Disclosures:
Pujan Kandel indicated no relevant financial relationships.
Deepa Wosti indicated no relevant financial relationships.
Murtaza Hussain indicated no relevant financial relationships.
Dipesh Rohita indicated no relevant financial relationships.
Frank Lukens indicated no relevant financial relationships.
Bhaumik Brahmbhatt indicated no relevant financial relationships.
Pujan Kandel, MD1, Deepa Wosti, MBBS2, Murtaza Hussain, MD3, Dipesh Rohita, MBBS4, Frank Lukens, MD1, Bhaumik Brahmbhatt, MD1. E0276 - Mortality After Surgery of Non-Malignant Colorectal Polyps: A Study From National Inpatient Database, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.