Advocate Lutheran General Hospital Park Ridge, Illinois
Robert Mowery, DO, David H. Kruchko, DO, Marc Fine, MD Advocate Lutheran General Hospital, Park Ridge, IL
Introduction: Foreign body ingestion is often seen in children and the elderly. Food particles such as chicken or fish bones are the most often ingested foreign bodies; however, most patients do not recall ingestion. Clinically, most foreign bodies pass through the GI tract without issue, however, complications occur in roughly 1% of cases. Complications of foreign body ingestion include bleeding, bowel obstruction, and perforation. We present a case of a 95-year-old female presenting with bright red blood per rectum found to have foreign body impaction with ulceration in the rectosigmoid region.
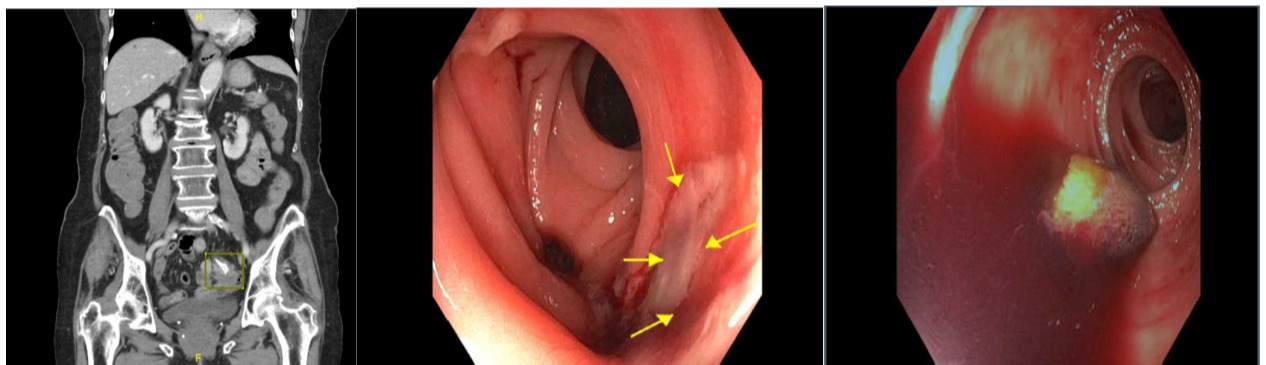
Case Description/Methods: A 95-year-old female with past medical history of diverticulosis and GERD presented with a complaint of rectal bleeding. She had experienced 7 episodes of voluminous bright red blood per rectum with diffuse crampy abdominal pain. She had no history of previous GI bleeds. Her most recent colonoscopy was 25 years prior with diverticulosis only. DRE was positive for bloody stool and her hemoglobin was 10g/dL with a baseline of approximately 13. CT scan showed rectosigmoid wall thickening consistent with inflammation, diverticula and a metallic-like object in the proximal sigmoid colon (figure 1a). The patient was started on piperacillin-tazobactam and prepared for flexible sigmoidoscopy occurring next morning. Endoscopy revealed areas of multiple diverticula, surrounding ulceration and bleeding in the rectosigmoid colon (figure 1b); cold biopsy was taken of the ulceration. A foreign body was found in the sigmoid colon (figure 1c) and was successfully removed with a Roth Net. The foreign body appeared to be swallowed chicken bone. Biopsy showed cellular debris and colonic mucosa with acute and chronic inflammation. Pathology identified the object as a bone fragment.
Discussion: The differential diagnosis of gastrointestinal bleeding is broad, but rarely is foreign body obstruction in the rectosigmoid region considered. The object must traverse 25 feet of small bowel prior to ulcerating the colon. The most common sites of complication occur at the ileocecal and rectosigmoid regions due to luminal narrowing and anatomic angulation. If complication occurs, 10-20% of foreign bodies can be removed endoscopically; 1% or less require surgical intervention. Intestinal strictures, cancer, diverticular disease, and hernias increase risk of complications after foreign body ingestion. Diverticulosis was the only identifiable risk factor in our patient case making it a unique clinical presentation.
Figure: Images from left to right Figure 1a foreign body as seen on admission CT Figure 1b sigmoid colon ulceration with diverticula seen proximal Figure 1c foreign body as seen on approach
Disclosures:
Robert Mowery indicated no relevant financial relationships.
David Kruchko indicated no relevant financial relationships.
Marc Fine indicated no relevant financial relationships.
Robert Mowery, DO, David H. Kruchko, DO, Marc Fine, MD. C0347 - Severe Rectal Bleeding due to Foreign Body Ingestion, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.