Pooja M. Jotwani, MD, Sachi Singhal, MD Crozer Chester Medical Center, Upland, PA
Introduction: Systemic Lupus Erythematosus (SLE) is a chronic inflammatory autoimmune disease that can have gastrointestinal manifestations related to immune complex deposition and vasculitis. Symptoms are non-specific and include abdominal pain and diarrhea.
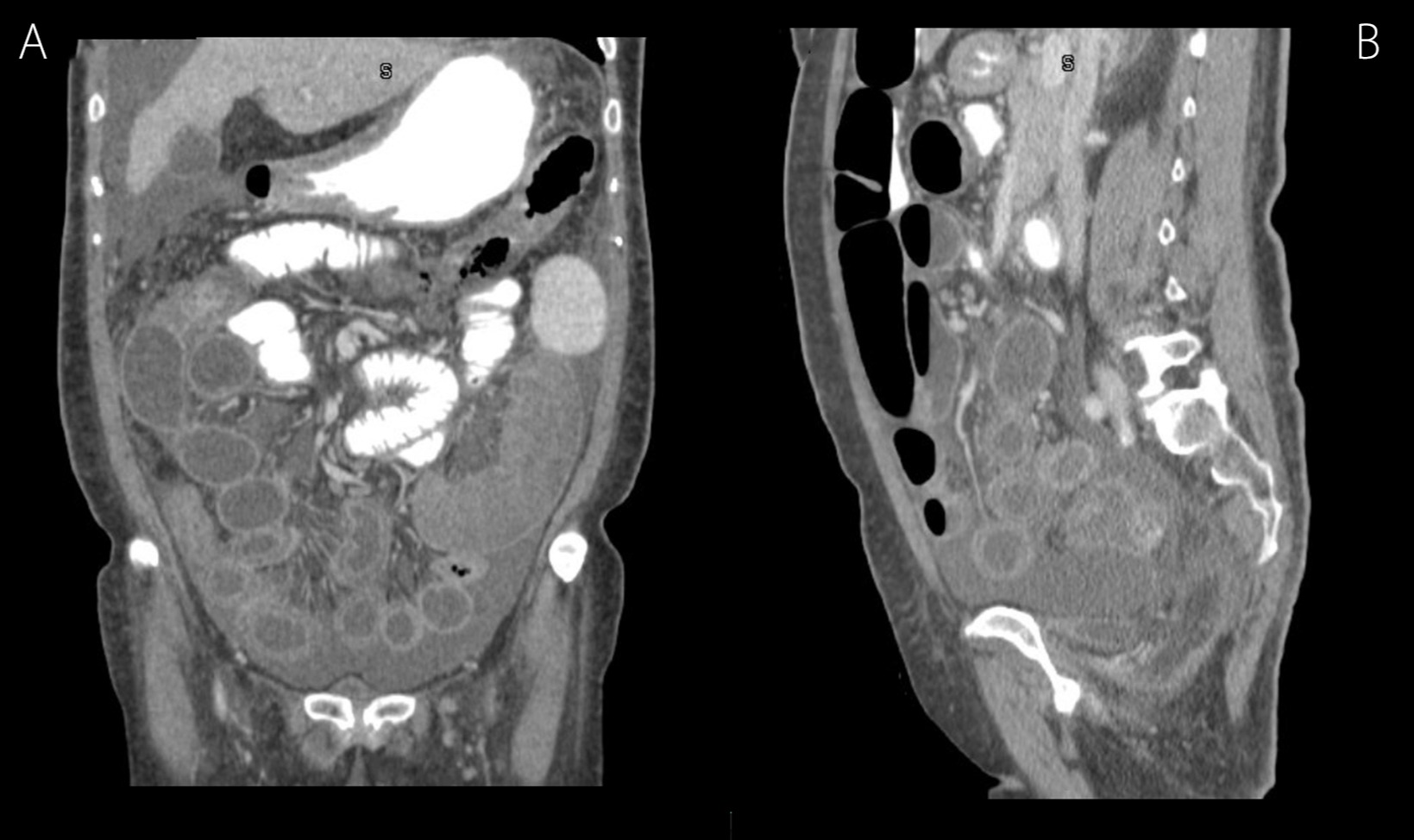
Case Description/Methods: A 66-year-old Asian woman with no prior medical history presented to the hospital with two months of generalized abdominal pain, nausea and watery diarrhea for 2 months. She reported a 10 lb unintentional weight loss. Initial labs revealed hemolytic anemia that was coombs positive with hemoglobin of 6.5 g/dL, as well as proteinuria. Contrast-enhanced CT of the abdomen & pelvis revealed moderate ascites, with normal appearing liver. Additionally evident was diffuse mural thickening of the descending colon, sigmoid colon, with the distal jejunum and ileum demonstrating “target signs” (Fig 1A & B). Stool studies were negative for infectious etiology. Upper endoscopy and colonoscopy revealed esophagitis, gastritis but normal appearing duodenum and colon. Single balloon enteroscopy revealed mild jejunitis and ulceration with biopsies suggesting chronic inflammation. Biopsies were negative for amyloidosis. Paracentesis revealed a serum ascites albumin gradient (SAAG) of < 1.1. She met the SLICC criteria for a diagnosis of SLE with coombs positive hemolytic anemia, positive ANA titer of 1:1280, anti ds-DNA titer 1:320, low completement levels and ascites. Her radiologic and endoscopic findings were attributed to lupus related enterocolitis. She was begun on intravenous methylprednisolone. Her symptoms progressively improved, after which steroids were tapered and she was transitioned to hydroxychloroquine therapy.
Discussion: We report here a case of enterocolitis as the initial presentation of SLE. Mesenteric vasculitis is the underlying mechanism, and patient can develop ascites as well as noted in our patient. Common sites of bowel involvement are the jejunum (80%) and the ileum (85%). Symptoms are generally non-specific. CT imaging has become the gold standard in diagnosis with findings of bowel wall edema (“target sign”) and engorgement of mesenteric vessels (“combs sign”). Lupus enterocolitis occurs in the setting of active SLE, and is visualized endoscopically as ischemic enteritis or chronic colonic ulcerations. This disease demonstrates favorable response to steroids. Early suspicion and prompt management is essential to prevent complications such as bowel ischemia or perforation.
Figure: Computerized tomography of the abdomen & pelvis in coronal [A] and sagittal views [B] demonstrated diffuse mural thickening of the jejunum and ileum in a “target sign” pattern.
Disclosures:
Pooja Jotwani indicated no relevant financial relationships.
Sachi Singhal indicated no relevant financial relationships.
Pooja M. Jotwani, MD, Sachi Singhal, MD. B0676 - Enterocolitis as the Initial Presentation of Systemic Lupus Erythematosus, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.