A0002 - Benefits of Early Cholecystectomy in Patients Presenting With Acute Gallstone Cholangitis Following ERCP: A Systematic Review and Meta-Analysis
Judie Hoilat, MD1, Mohamad F. Ayas, MD2, Dayana Nasr, MD3, Abdul Haseeb, MD1 1Loyola University Medical Center, Maywood, IL; 2Ascension St. John Hospital, Detroit, MI; 3SUNY Upstate University Hospital, Syracuse, NY
Introduction: The mainstay of management of acute gallstone cholangitis includes intravenous fluid resuscitation, appropriate antibiotic coverage, biliary drainage, and subsequent cholecystectomy. Even though cholecystectomy following an episode of gallstone associated cholangitis is strongly supported in the literature, the exact timing of cholecystectomy remains uncertain. Delay in cholecystectomy after the diagnosis of acute cholangitis may increase the risk of recurrent emergency department visits and hospital admissions. This systematic review aims to evaluate and compare the advantages, safety and efficacy of early cholecystectomy in patients with acute cholangitis.
Methods: A systematic review and meta-analysis was carried out according to the PRISMA and Cochrane Handbook for Systematic Review of Interventions. Six databases (PubMed, Scopus, Embase, Google Scholar, Web of Science, and Cochrane Central Register of Controlled Trials) were screened from inception until 01-May-2022. The inclusion criteria comprised all randomized controlled trials (RCTs) and nonrandomized comparative trials (NCTs) that evaluated early versus late cholecystectomy among patients with acute cholangitis. The efficacy outcomes were summarized as mean difference (MD) or risk ratio (RR) with 95% confidence interval (CI).
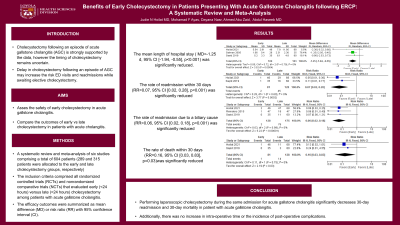
Results: Six studies met the inclusion criteria, comprising a total of 604 patients (289 and 315 patients were allocated to the early and late cholecystectomy groups, respectively). The mean length of hospital stay (MD=-1.25 d, 95% CI [-1.94, -0.55], p< 0.001), rate of readmission within 30 days (RR=0.07, 95% CI [0.02, 0.28], p< 0.001), rate of readmission due to a biliary cause (RR=0.06, 95% CI [0.02, 0.18], p< 0.001), and rate of death within 30 days (RR=0.16, 95% CI [0.03, 0.83], p=0.03) were significantly reduced in favor of the early cholecystectomy group compared with the late cholecystectomy group.
Discussion: Performing cholecystectomy during the same admission for acute gallstone cholangitis was associated with a lower 30-day readmission rate and 30-day mortality rate. Additionally, there was no increase in operative time or the incidence of post-operative complications.
Figure: Figure 1. Meta-analysis of the efficacy endpoints: (a) mean length of hospital stay, (b) rate of readmission within 30 days, (c) rate of death within 30 days, (d) rate of postoperative complications.
Disclosures:
Judie Hoilat indicated no relevant financial relationships.
Mohamad Ayas indicated no relevant financial relationships.
Dayana Nasr indicated no relevant financial relationships.
Abdul Haseeb indicated no relevant financial relationships.
Judie Hoilat, MD1, Mohamad F. Ayas, MD2, Dayana Nasr, MD3, Abdul Haseeb, MD1. A0002 - Benefits of Early Cholecystectomy in Patients Presenting With Acute Gallstone Cholangitis Following ERCP: A Systematic Review and Meta-Analysis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.