San Antonio Uniformed Services Health Education Consortium San Antonio, TX
William M. LaShomb, MD1, Cody Ashcroft, MD2, Jerome C. Edelson, MD3, John Magulick, MD1 1San Antonio Uniformed Services Health Education Consortium, San Antonio, TX; 2Brooke Army Medical Center, Fort Sam Houston, TX; 3Brooke Army Medical Center, San Antonio, TX
Introduction: Patients with a Roux-en-Y hepaticojejunostomy (RYHJ) present a unique challenge when endoscopic retrograde cholangiography (ERC) is required. Standard approaches range from a surgical approach involving laparoscopic assistance to device assisted enteroscopy, with transoral approaches generally being variably successful, due to anatomy, length of intestinal limbs after surgery, and limitations in available accessories for use in device assisted enteroscopy. Here, we report the endoscopic use of a LAMS to create a duodenojejunostomy (DJ), thereby enabling ERC in a patient with RYHJ.
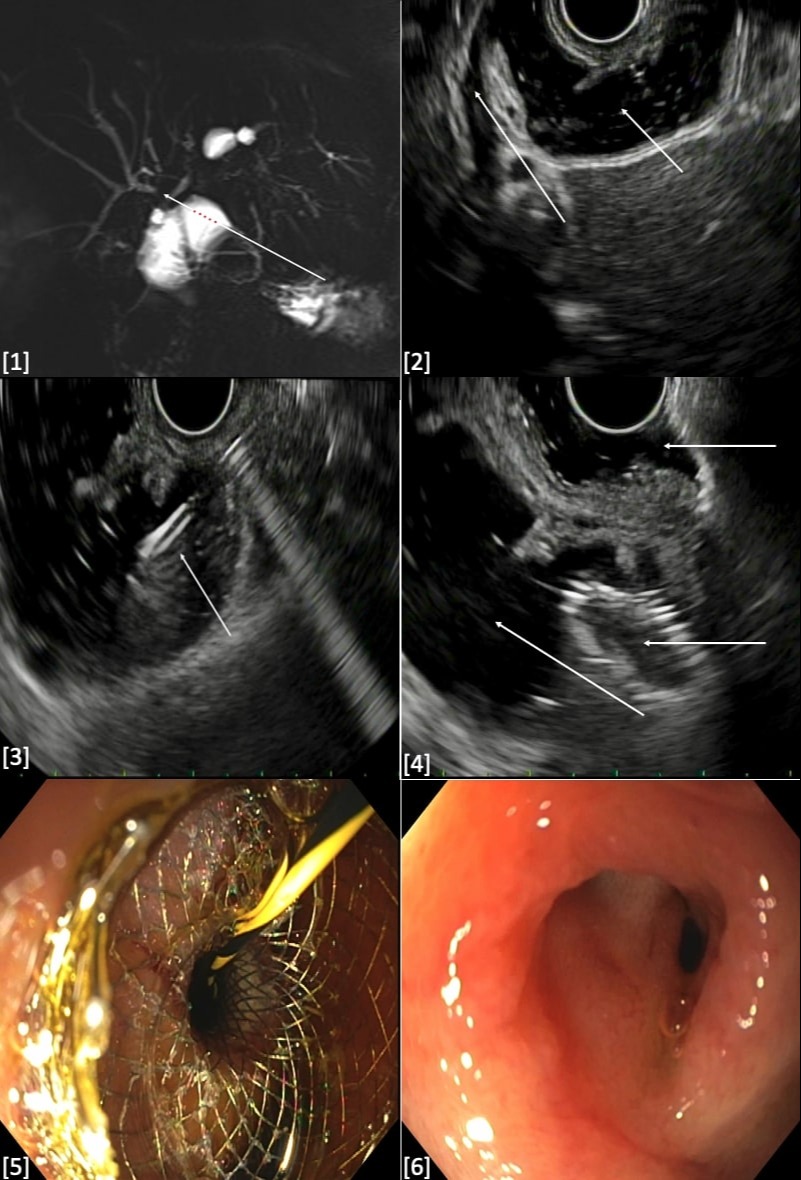
Case Description/Methods: A 46-year-old woman status post cholecystectomy complicated by common bile duct injury necessitating RHYJ and prior anastamotic strictures, presented with recurrent self-limited cholangitis. She presented to clinic with intermittent episodes right upper quadrant pain, and fever which were treated conservatively with antibiotics. MRCP demonstrated stricture of the hepatic duct near the anastomosis [1]. Device assisted endoscopy was performed, but the anastomosis was unable to be reached. After discussing endoscopic, IR, and surigcal options we proceeded with EUS guided interventions given the anticipated need for recurrent interventions for a biliary stricture.
EUS demonstrated mild intrahepatic dilation with limited access points for hepaticogastrostomy. The bile duct and hepaticojejunostomy were visualized from the bulb with small bowel adjacent to the anastomosis [2]. The jejunum was accessed using a 19 G FNA needle, and bile was aspirated to confirm intraluminal location. The jejunum was filled with 200 mL of sterile water and contrast [3]. A 15 mm x 10 mm AXIOS was then deployed in good position, creating a DJ, which was confirmed fluoroscopically and endoscopically [4]. Contrast was then injected through the stent to exclude a leak.
4 weeks later, ERCP was performed via the DJ [5]. Cholangioscopy was performed which showed some edematous bile duct mucosa without findings concerning for malignancy [6]. Biopsies and brushings were performed and three plastic stents were placed. The patient tolerated the procedure well, the tissue was benign and the patient has had resolution of her cholangitis symptoms.
Discussion: In conclusion, we report a novel use of LAMS enabling ERC in patient’s status post RHYJ which allows easy access for repeat interventions and avoids the difficulties and limitations of device assisted enteroscopy ERCP.
Figure: Image 1. MRCP showing hepatic duct stricture near the anastomosis Image 2. EUS with bile duct adjacent to fluid filled jejunum Image 3. EUS with FNA needle accessing hepaticojejunostomy Image 4. EUS with LAMS deployed from duodenum to jejunum Image 5. Matured duodenojejunostomy Image 6. Cholangioscopy demonstrating edematous mucosa
Disclosures:
William LaShomb indicated no relevant financial relationships.
Cody Ashcroft indicated no relevant financial relationships.
Jerome Edelson indicated no relevant financial relationships.
John Magulick indicated no relevant financial relationships.
William M. LaShomb, MD1, Cody Ashcroft, MD2, Jerome C. Edelson, MD3, John Magulick, MD1. A0439 - ERCP via EUS Guided Duodenojejunostomy for a Biliary Stricture After Roux-en-Y Hepaticojejunostomy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.