Julianna Tantum, DO, Nadia Al Haddad, MD, Romy Chamoun, MD, Michael Choe, MD Lankenau Medical Center, Wynnewood, PA
Introduction: Pembrolizumab is an anti-programmed cell death (PD-1) receptor inhibitor that is commonly used for the treatment of small-cell lung cancer (SCLC). This checkpoint inhibitor has been associated with numerous immune-related side effects, including colitis, vasculitis, myocarditis, and hepatitis. We report a case of pembrolizumab-induced liver injury in a SCLC patient that was successfully treated with steroids.
Case Description/Methods: This is a 74-year-old female with a history of SCLC who presented to the hospital with abnormal liver function tests (LFTs) on outpatient labs. She had a 2-month history of jaundice, fatigue, lower extremity weakness, and generalized malaise. Her last pembrolizumab infusion was 10 days prior. On admission, she was hemodynamically stable. Labs were notable for AST 1,211 IU/L, ALT 674 IU/L, alkaline phosphatase 1,216 IU/L, total bilirubin 13.8 mg/dL, direct bilirubin 8.8 mg/dL, total CK 4,474 U/L. Serum ethanol and acetaminophen levels were negative. Imaging was unremarkable (Image 1A). She was treated with N-acetylcysteine, ceftriaxone & metronidazole, and methylprednisolone 60mg IV daily. Acute hepatitis panel, hepatitis C antibody, ANA, LKM-1 antibody, IGG subclass, and anti-mitochondrial antibody were negative. Smooth muscle antibody (SM-Ab) was positive with titer 1:40. Four days after admission, her labs worsened. MRCP was unremarkable (Image 1B). Methylprednisolone was increased to 100mg daily with improvement in her LFTs after 3 days. She was changed to prednisone 80mg daily and was discharged on a steroid taper with normalization of her LFTs 1 month later. Due to the temporal relationship with her infusion, her SM-Ab positivity was not representative of autoimmune hepatitis but rather of drug induced liver injury.
Discussion: Immune-mediated hepatitis is one of the most common and serious side effects of pembrolizumab. Severe elevations of LFTs, such as in our patient, are uncommon, occurring in about 1% of patients. It is postulated that anti-PD-1 antibodies remain attached to lymphocytes weeks after the last infusion, which can cause hepatitis after discontinuation or long after initiation of therapy. Most cases resolve with treatment, including immunosuppressants and corticosteroids, but immune-mediated hepatitis related deaths have been reported. After resolution, most patients can restart therapy with close monitoring but often require concomitant immunosuppressant therapy.
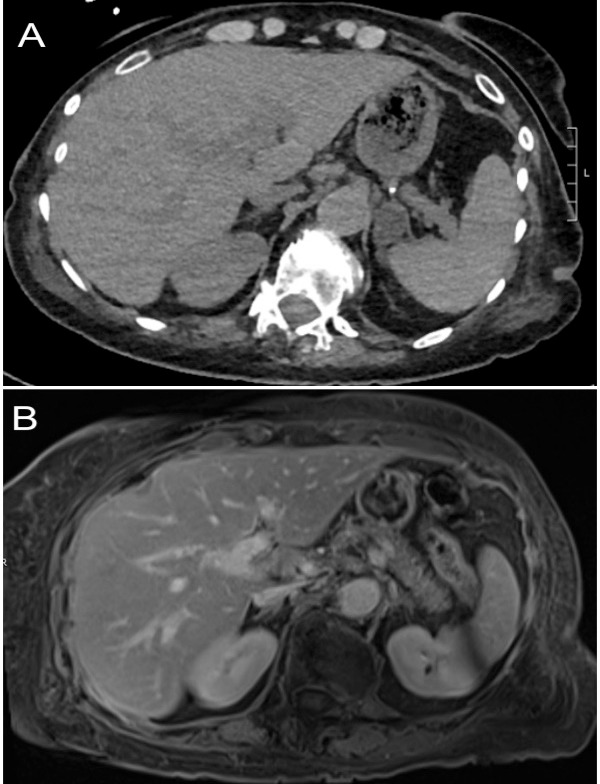
Figure: Image 1A. Computed Tomography (CT) abdomen and pelvis with intravenous contrast showing a collapsed but thickened gallbladder with trace pericholecystic fluid, no biliary ductal dilation, mild periportal edema. 1B. Magnetic resonance cholangiopancreatography (MRCP) showing no intrahepatic or common bile ductal dilation or stricture, no choledocholithiasis, normal liver size, and periportal edema.
Disclosures:
Julianna Tantum indicated no relevant financial relationships.
Nadia Al Haddad indicated no relevant financial relationships.
Romy Chamoun indicated no relevant financial relationships.
Michael Choe indicated no relevant financial relationships.
Julianna Tantum, DO, Nadia Al Haddad, MD, Romy Chamoun, MD, Michael Choe, MD. A0535 - Positive Smooth Muscle Antibodies in a Patient With Pembrolizumab-Induced Liver Injury, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.