Spyridon Zouridis, MD1, Omar Tageldin, MD1, Nour Parsa, MD2 1Albany Medical Center, Albany, NY; 2Loma Linda University Medical Center, Loma Linda, CA
Introduction: Gastric malignancies often present with anorexia, nausea, abdominal pain, early satiety, dysphagia and weight loss. Gastrointestinal bleeding and metastatic disease can further complicate the presentation. When the underlying disease has progressed, clinicians may encounter unusual signs and symptoms such as in this rare patient case. Moreover, patients may omit to report typical symptoms, hence a high clinical suspicion should be maintained by the clinician.
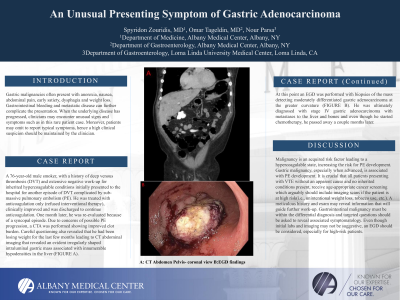
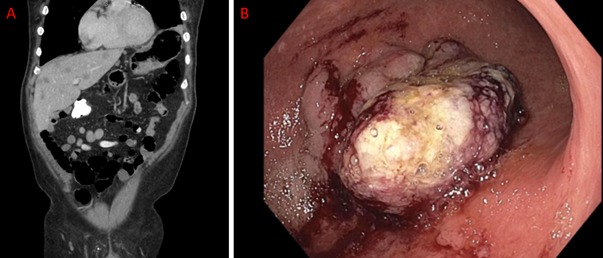
Case Description/Methods: A 76-year-old male smoker, with a history of deep venous thrombosis (DVT) and extensive negative work-up for inherited hypercoagulable conditions initially presented to the hospital for another episode of DVT complicated by sub-massive pulmonary embolism (PE). He was treated with anticoagulation only (refused interventional therapy), clinically improved and was discharged to continue anticoagulation. One month later, he was re-evaluated because of a syncopal episode. Due to concerns of possible PE progression, a CTA was performed showing improved clot burden. Careful questioning also revealed that he had been losing weight for the last few months leading to CT abdominal imaging that revealed an evident irregularly shaped intraluminal gastric mass associated with innumerable hypodensities in the liver (FIGURE A). At this point an EGD was performed with biopsies of the mass detecting moderately differentiated gastric adenocarcinoma at the greater curvature (FIGURE B). He was ultimately diagnosed with stage IV gastric adenocarcinoma with metastases to the liver and bones and even though he started chemotherapy, he passed away a couple months later.
Discussion: Malignancy is an acquired risk factor leading to a hypercoagulable state, increasing the risk for PE development. Gastric malignancy, especially when advanced, is associated with PE development. It is crucial that all patients presenting with VTE without an apparent cause and no inherited conditions present, receive age-appropriate cancer screening which arguably should include imaging scans if the patient is at high risk (i.e., unintentional weight loss, tobacco use, etc.). A meticulous history and exam may reveal information that will guide further work-up. Gastrointestinal malignancy must be within the differential diagnosis and targeted questions should be asked to reveal associated symptomatology. Even though initial labs and imaging may not be suggestive, an EGD should be considered, especially for high-risk patients.