East Carolina University/Vidant Medical Center Greenville, NC
Daniyal Abbas, MD1, Shiva Poola, MD2, Marwan Majeed, MD, MPH3, Kara Regan, MD2 1East Carolina University/Vidant Medical Center, Greenville, NC; 2ECU Health Medical Center/Brody School of Medicine, Greenville, NC; 3East Carolina University, Greenville, NC
Introduction: Sarcoidosis is a rare, systemic disease that can affect any organ but is most associated with pulmonary manifestations. Excluding the liver, gastrointestinal involvement of sarcoidosis is rare. PS can masquerade as underlying malignancy which poses a diagnostic and therapeutic challenge. Clinical presentation includes symptoms secondary to pancreatic duct obstruction or pancreatic parenchymal infiltration from enlarged lymph nodes that can result in abdominal pain, jaundice, weight loss, and nausea or emesis. However, these non-specific symptoms can be present in patients with pancreatitis or malignancy. This case highlights the rare finding of pancreatic sarcoidosis masquerading as a pancreatic adenocarcinoma
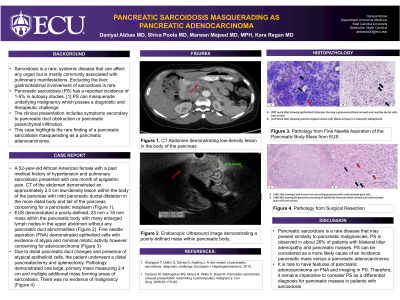
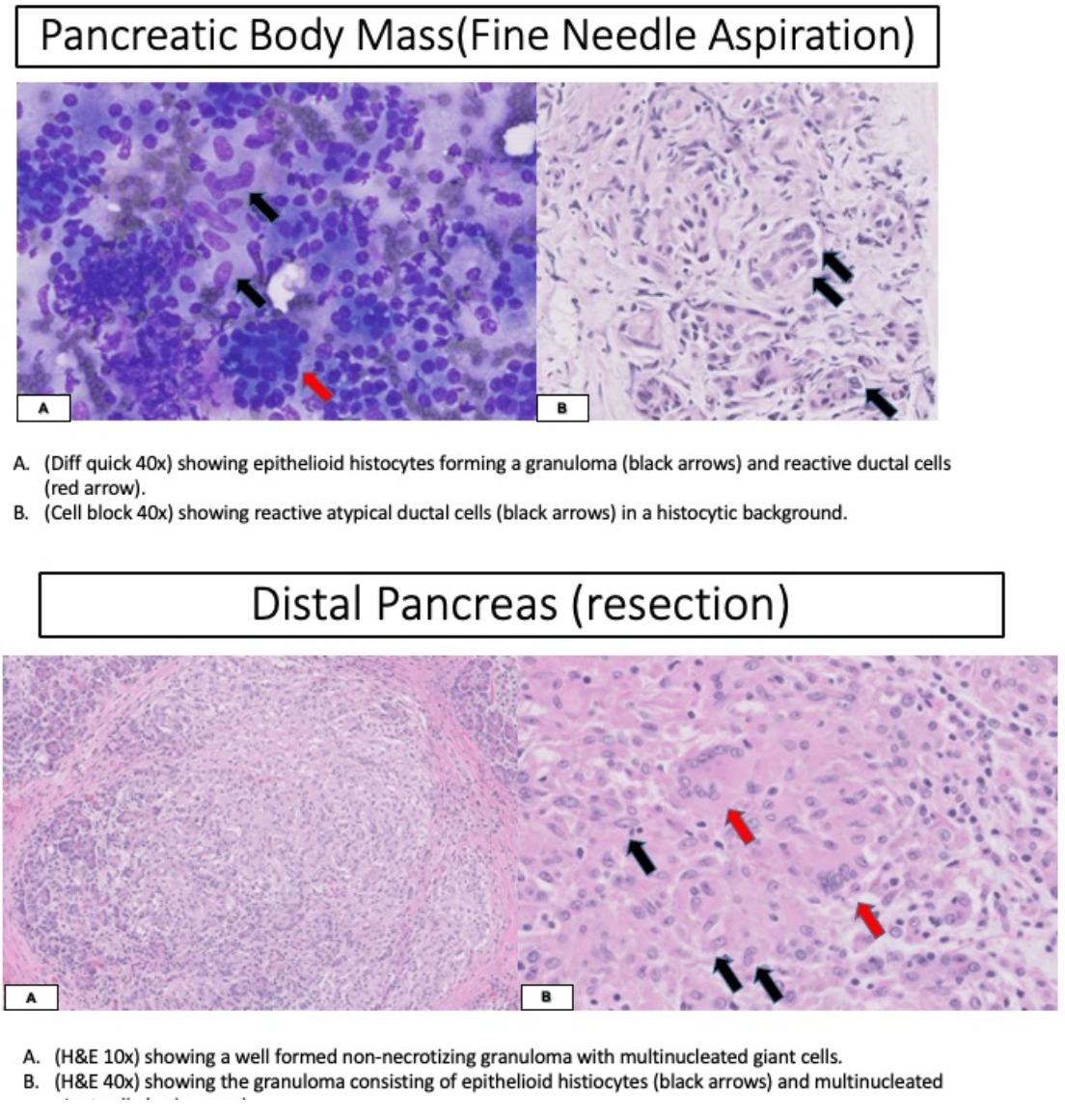
Case Description/Methods: A 52-year-old African American female with a past medical history of hypertension and pulmonary sarcoidosis presented with one month of epigastric pain. She denied any fatigue, early satiety, diarrhea, nausea, vomiting, obstructive symptoms, or unexpected weight loss. Computed tomography (CT) of the abdomen demonstrated an approximately 2.0 cm low-density lesion within the body of the pancreas with mild pancreatic ductal dilatation in the more distal body and tail of the pancreas concerning a pancreatic neoplasm. She underwent additional imaging for staging including a CT chest that demonstrated cervical lymphadenopathy and progressive hilar adenopathy consistent with her history of pulmonary sarcoidosis. She underwent endoscopic ultrasound which demonstrated a poorly defined 23 mm x 18 mm mass within the pancreatic body with many enlarged lymph nodes in the upper abdomen without any pancreatic duct abnormalities. Fine needle aspiration (FNA) demonstrated epithelioid cells with evidence of atypia and minimal mitotic activity; however, concerning for an adenocarcinoma (Fig 1). Given the concern of an underlying neoplastic process secondary to distal pancreatic duct changes and the presence of atypical epithelioid cells, the patient underwent a distal pancreatectomy and splenectomy. Pathology demonstrated one large, primary mass measuring 2.4 cm and multiple additional masses forming areas of sarcoidosis. There was no evidence of malignancy. Her postoperative course was uncomplicated with plans for surveillance imaging in 1 year.
Discussion: Although most cases of PS are asymptomatic, the risk of an underlying malignancy needs to be weighed against the risk of PS. Sharing this knowledge with patients can help guide decision-making.
Figure: Figure 1. Histologic analysis of the distal pancreatectomy and splenectomy specimen demonstrating no evidence of malignancy
Disclosures:
Daniyal Abbas indicated no relevant financial relationships.
Shiva Poola indicated no relevant financial relationships.
Marwan Majeed indicated no relevant financial relationships.
Kara Regan indicated no relevant financial relationships.
Daniyal Abbas, MD1, Shiva Poola, MD2, Marwan Majeed, MD, MPH3, Kara Regan, MD2. B0033 - Pancreatic Sarcoidosis Masquerading as Pancreatic Adenocarcinoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.