Teresa Da Cunha, MD, Jaimy Villavicencio Kim, MD, Haleh Vaziri, MD UConn Health, Farmington, CT
Introduction: Internal gastrointestinal (GI) fistulas can occur between different segments of the GI tract or between the GI tract and another nearby structure. Most of these arise due to a surgical complication or occasionally from an inflammatory process, such as IBD. Rarely, malignant tumors can erode to the GI tract forming a tumor-bowel fistula (TBF). We describe a patient with late-stage renal cell carcinoma (RCC) presenting with persistent fevers and diarrhea secondary to a TBF.
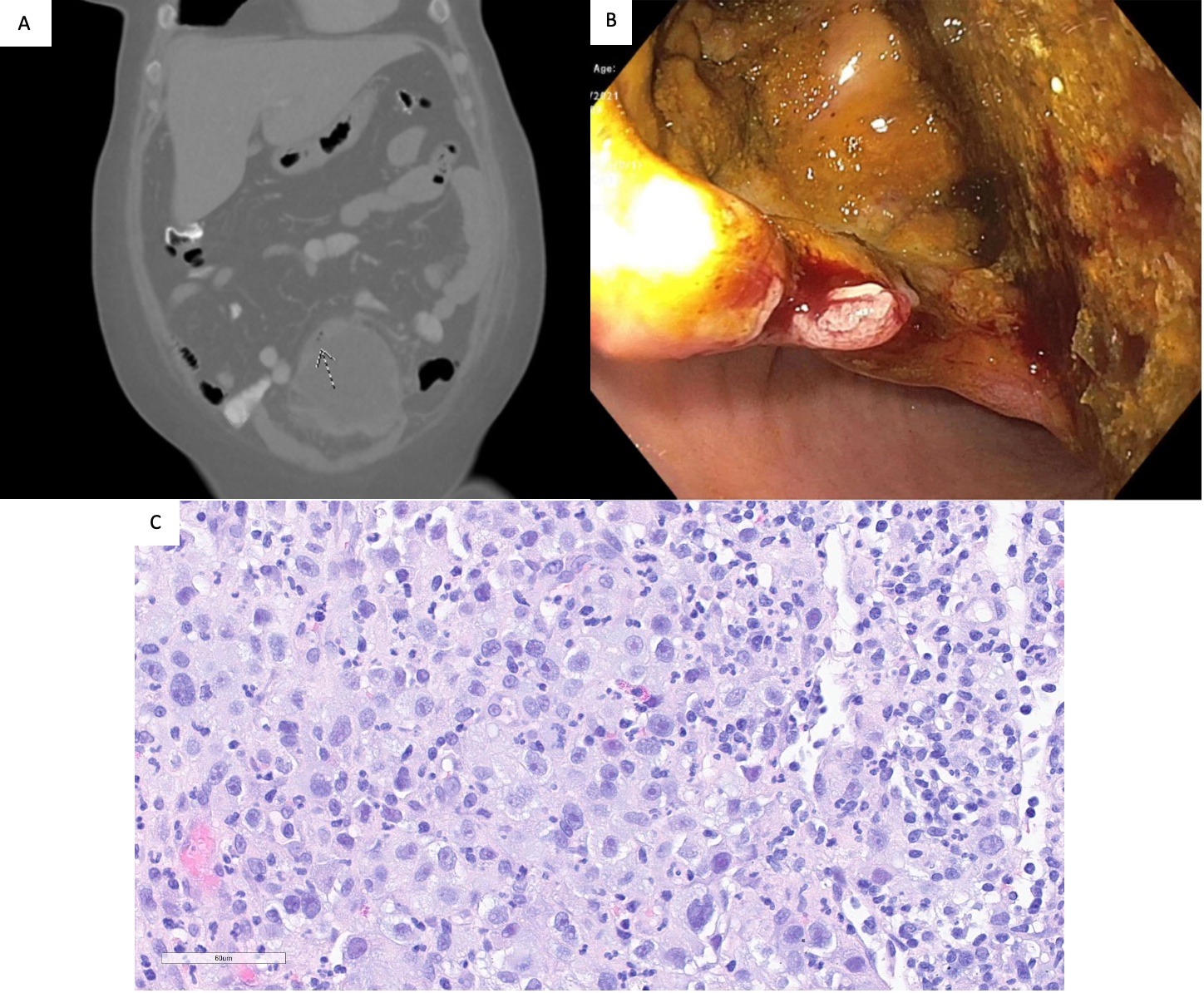
Case Description/Methods: A 55-year-old female with metastatic renal cell carcinoma, presented to the ER with one week of fever, abdominal discomfort, and non-bloody diarrhea. She denied nausea, vomiting, sick contacts or recent travel. On arrival she was febrile (101.4 F), heart rate of 143 bpm. The reminder of the physical exam was unremarkable. Laboratory results revealed a WBC of 52.9 x 109 /L. A chest x-ray did not show signs of infection. Vancomycin and piperacillin/tazobactam were initiated. Blood, urine and stool cultures, fecal calprotectin and Clostridium difficile tests were negative. CT scan of the abdomen and pelvis showed a necrotic mass in the left aspect of the pelvis that appeared to erode the sigmoid colon (Fig.1A). A sigmoidoscopy revealed a 2 cm area in the sigmoid colon with direct communication to a mass that was biopsied (Fig.2B). The pathology findings were consistent with RCC (Fig.2C). A transverse colostomy with mucous fistula was successful. She completed 14 days of antibiotic therapy and the fever resolved. Five months later she has had no complications and continued treatment with immunotherapy and radiation.
Discussion: GI involvement by RCC is very rare and mostly occurs by metastatic spread to the small bowel. Approximately 5-15% of RCCs spread to nearby structures and 20-30% of patients have metastasis at the time of diagnosis. Formation of a TBF might occur spontaneously from tumor eroding to the bowel or as a consequence of chemotherapy and/or radiotherapy. Due to the retroperitoneal location of the kidney, the colon is almost never affected. From rare reported cases, patients mainly present with lower GI bleeding. In our patient, migration of colonic contents to the tumor mass via TBF may have led to superinfection of the mass. In the presence of intra-abdominal tumors, especially several metastatic masses, the presence of fever can be a sign of TBF and appropriate imaging with CT scan and careful endoscopic examination are necessary to establish a diagnosis and guide the surgical management.
Figure: Fig 1. (A) CT scan of the abdomen and pelvis shows a necrotic mass in the left aspect of the pelvis that appears to erode the wall of the sigmoid colon; (B) Flexible sigmoidoscopy revealing a 2 cm erosion of the sigmoid colon with direct communication to the mass; (C) H&E image of the colon biopsy. The large cells with variably sized nuclei, sometimes prominent nucleoli and abundant eosinophilic cytoplasm form a sheet of neoplastic cells. On the right-hand side of the image the smaller cells are plasma cells and lymphocytes with a few neutrophils.
Disclosures:
Teresa Da Cunha indicated no relevant financial relationships.
Jaimy Villavicencio Kim indicated no relevant financial relationships.
Haleh Vaziri indicated no relevant financial relationships.
Teresa Da Cunha, MD, Jaimy Villavicencio Kim, MD, Haleh Vaziri, MD. B0160 - Tumor-Colonic Fistula in a Patient With Renal Cell Carcinoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.