Haroon Alam, MS1, Rohma Qureshi, MS2, Asad Jehangir, MD3, Zain A. Sobani, MD4, Amanda Barrett, MD5, John Erikson L. Yap, MD6, Kenneth J. Vega, MD, FACG6, Viveksandeep Chandrasekar, MBBS6 1Medical College of Georgia at Augusta University, Augusta, GA; 2Shalamar Medical & Dental College, Lahore, Punjab, Pakistan; 3MD, Augusta, GA; 4Augusta University/Medical College of Georgia, Augusta, GA; 5Augusta University Medical College of Georgia, Augusta, GA; 6Augusta University Medical College of Georiga, Augusta, GA
Introduction: New onset dysphagia warrants endoscopic evaluation to rule out structural etiologies, including malignancy. The vast majority ( >95%) of esophageal cancers are adenocarcinoma or squamous cell carcinoma. We report a rare case of esophageal small-cell neuroendocrine carcinoma (NEC) presenting with dysphagia.
Case Description/Methods: A 76-year-old African American female with a history of left lung non-small cell neoplasm status post left lower lobectomy and adjuvant chemo-radiation presented to an outside hospital with dysphagia to solids and unintentional weight loss over the previous month. She denied history of smoking. Her BP was 163/81, pulse 81, temperature 36.7 and respiratory rate 16. Rest of the physical exam was normal. Laboratory tests showed mild normocytic anemia (hemoglobin 11.2 g/dL). Chest CT scan revealed a soft tissue mass at junction of the cervical and thoracic esophagus (Figure 1A). Due to the proximity of the mass to the airway, she was transferred to our hospital for evaluation. EGD confirmed an esophageal mass located at 16 cm from incisors, just distal to the upper esophageal sphincter, causing near complete esophageal obstruction (Figures 1B-C). Using a pediatric gastroscope, the mass was traversed and noted to extend to 25 cm from the incisors. Multiple biopsies were obtained with histology showing small cell NEC (Figures 1D-F). Positron emission tomography revealed lymph nodes metastases above and below the diaphragm, liver and multiple bones. Brain magnetic resonance imaging was negative for metastases. Patient was not a candidate for surgical resection or stenting given the proximal esophageal location of the tumor and required gastrostomy tube placement for nutrition by interventional radiology. Palliative chemoradiation (carboplatin, etoposide, atezolizumab) has started and the patient is currently tolerating therapy for 2 months since diagnosis.
Discussion: Esophageal small-cell NEC is a rare esophageal malignancy, accounting for 0.4-2.0% of esophageal cancers. Esophageal small-cell NEC are typically highly aggressive, frequently have metastasized by the time of diagnosis, and associated with poor prognosis. While surgical resection may be attempted for limited disease, those with metastases are typically managed with chemotherapy, with or without radiotherapy. Gastroenterologists should include rare esophageal malignancies, including small cell NEC, on their differential for new onset dysphagia to solids.
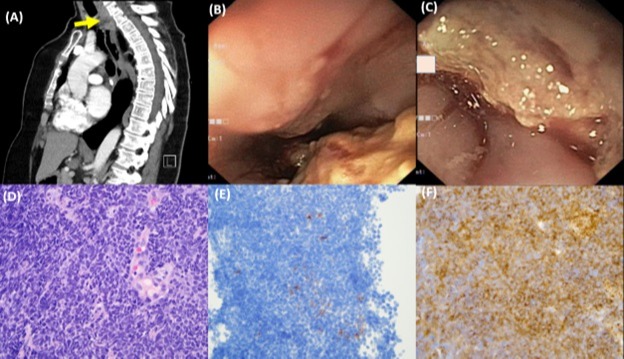
Figure: Figure 1A: Computerized tomography scan of the chest (sagittal view) showing a soft tissue mass at the junction of the cervical and thoracic esophagus (arrow). Figure 1B-C: Esophagogastroduodenoscopy showing an esophageal mass located at 16 cm from incisors causing near complete obstruction of the esophagus. Figure 1D: A high power (400x, H&E) view shows a highly cellular tumor comprised of basophilic cells, with scant cytoplasm, high nuclear/cytoplasmic ratio, salt-and pepper chromatin, and nuclear molding with crush artifact. There are abundant apoptotic cells and frequent mitotic figures, indicating a highly proliferative tumor. Figure 1E: 400x, chromogranin immunostaining, showing focally positive cells, consistent with neuroendocrine differentiation. Figure 1F: 400x, synaptophysin immunostaining, showing diffuse positivity in tumor cells, consistent with neuroendocrine differentiation.
Disclosures:
Haroon Alam indicated no relevant financial relationships.
Rohma Qureshi indicated no relevant financial relationships.
Asad Jehangir indicated no relevant financial relationships.
Zain Sobani indicated no relevant financial relationships.
Amanda Barrett indicated no relevant financial relationships.
John Erikson Yap indicated no relevant financial relationships.
Kenneth Vega indicated no relevant financial relationships.
Viveksandeep Chandrasekar indicated no relevant financial relationships.
Haroon Alam, MS1, Rohma Qureshi, MS2, Asad Jehangir, MD3, Zain A. Sobani, MD4, Amanda Barrett, MD5, John Erikson L. Yap, MD6, Kenneth J. Vega, MD, FACG6, Viveksandeep Chandrasekar, MBBS6. A0238 - Small Cell Neuroendocrine Esophageal Carcinoma: A Rare Cause of Dysphagia, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.