Tulane University School of Medicine New Orleans, Louisiana
Kyle A. Jones, MD, Behnam Laderian, MD, Benjamin Guider, MD Tulane University School of Medicine, New Orleans, LA
Introduction: Enteropathy associated T cell lymphoma (EATL) is a rare condition accounting for less than 5% of gastrointestinal lymphomas. This disease is difficult to diagnose in the early stages with most patients being diagnosed at stage IV. Presenting symptoms include abdominal pain, weight loss, fatigue, fevers, and night sweats. Given the overlap of symptomatology with Crohn’s disease (CD), diagnosis of EATL can be delayed.
Case Description/Methods: A 56 year-old man arrived with fevers, chills, and diarrhea for 3 months. Exam was notable for mild abdominal tenderness. Labs showed a WBC of 43K, positive C diff toxin, elevated fecal calprotectin, elevated CRP to 23, and negative tissue transglutaminase. CT abdomen showed terminal ileitis and colitis. The patient was treated with oral vancomycin with improvement of his diarrhea.
Six months later the patient was seen in clinic. He was again having significant diarrhea, abdominal pain, fevers, chills, night sweats, and a 50-pound weight loss. Colonoscopy was significant for deep ulcerations of the terminal ileum. Biopsies showed chronic ileitis with ulceration and focal collections of epithelioid histiocytes suggestive of granulomas. There was no evidence of dysplasia or metaplasia seen on biopsy. Following the biopsy results the patient was diagnosed with CD.
One week later, he was admitted with weakness, fatigue, and worsening abdominal pain. CT enterography revealed an enteroenteric fistula. The patient underwent exploratory laparotomy with resection of the small intestine and end ileostomy. Pathology showed CD-30 positive T cell lymphoma indicating EATL. The background intestinal mucosa also revealed features suggestive of gluten-sensitive enteropathy with villous atrophy and increased intraepithelial lymphocytes.
Ultimately this patient was started on chemotherapy but died of complications related to chemotherapy, intra-abdominal abscesses, and renal failure less than 2 months following diagnosis of EATL.
Discussion: This case illustrates the difficulty in diagnosing EATL. Patient initially was diagnosed with CD given the clinical presentation and endoscopic findings. It was not until the patient underwent small bowel resection due to enteroenteric fistula that the diagnosis of EATL caused by gluten-sensitive enteropathy was made by pathology. Negative celiac serologies made this case a more challenging one. Although rare, EATL must be considered in the differential for patients presenting with similar symptomatology as patients suspected to have CD.
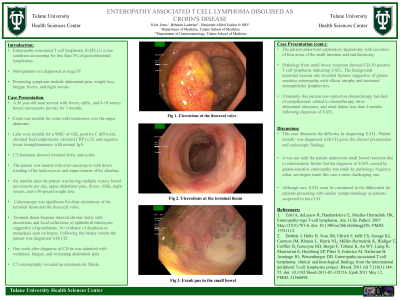
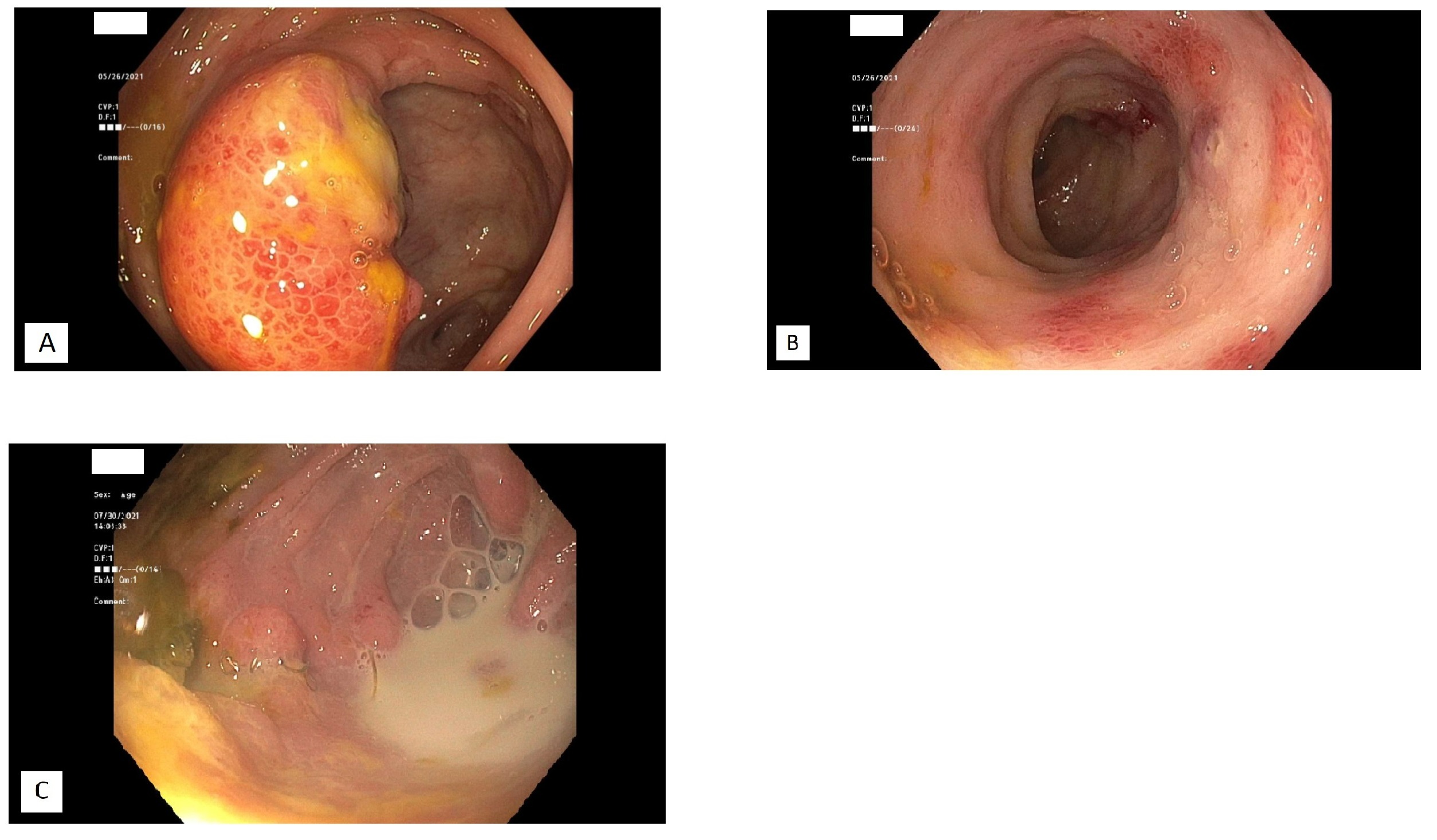
Figure: A: Ulcerations at the ileocecal valve B: Ulcerations at the terminal ileum C: Frank pus in the small bowel
Disclosures:
Kyle Jones indicated no relevant financial relationships.
Behnam Laderian indicated no relevant financial relationships.
Benjamin Guider indicated no relevant financial relationships.
Kyle A. Jones, MD, Behnam Laderian, MD, Benjamin Guider, MD. A0656 - Enteropathy Associated T-cell Lymphoma Disguised as Crohn's Disease, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.