Caileen Sennett, MD, Gres Karim, MD, Minira Aslanova, DO, Wan Lam, MD Mount Sinai Beth Israel, New York, NY
Introduction: Perforation of the cecum presents with lower quadrant abdominal pain that may be acute or subacute, depending on the level of containment. The cecum is one of the most common locations of perforation given it is the thinnest portion of the large intestine. Perforation of the cecum usually occurs due to neoplasm or diverticulitis. Iatrogenic causes with foreign body ingestion are rare causes of cecal perforation. We present a case of a 72-year-old male with acute, progressive right lower abdominal pain, found to have cecal perforation secondary to a foreign body ingestion.
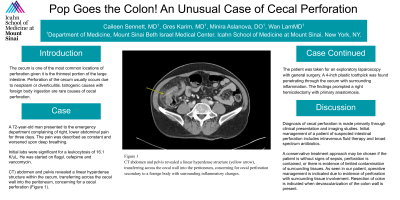
Case Description/Methods: A 72-year-old man presented to the emergency department complaining of right, lower abdominal pain for three days. The pain was described as constant and worsened upon deep breathing. He denied fever, chills, nausea, vomiting or hematochezia. Initial labs were significant for a leukocytosis of 16.1 K/uL. He was started on flagyl, cefepime and vancomycin. Computed Tomography (CT) abdomen and pelvis revealed a linear hyperdense structure within the cecum, transferring across the cecal wall into the peritoneum, concerning for a cecal perforation (Figure 1). The patient was taken for an exploratory laparoscopy with general surgery. A 4-inch plastic toothpick was found penetrating through the cecum with surrounding inflammation. The findings prompted a right hemicolectomy with primary anastomosis. The patient later admitted to swallowing a plastic toothpick. He was monitored closely post-operatively. Upon regaining bowel function and medical stability, he was discharged home.
Discussion: Diagnosis of cecal perforation is made primarily through clinical presentation and imaging studies. Initial management of a patient of suspected intestinal perforation includes intravenous fluid therapy and broad spectrum antibiotics. A conservative treatment approach may be chosen if the patient is without signs of sepsis, perforation is contained, or there is evidence of limited contamination of surrounding tissues. As seen in our patient, operative management is indicated due to evidence of perforation with surrounding tissue involvement. Resection of colon is indicated when devascularization of the colon wall is present.
Figure: Figure 1 CT abdomen and pelvis revealed a linear hyperdense structure (yellow arrow), transferring across the cecal wall into the peritoneum, concerning for cecal perforation secondary to a foreign body with surrounding inflammatory changes.
Disclosures:
Caileen Sennett indicated no relevant financial relationships.
Gres Karim indicated no relevant financial relationships.
Minira Aslanova indicated no relevant financial relationships.
Wan Lam indicated no relevant financial relationships.
Caileen Sennett, MD, Gres Karim, MD, Minira Aslanova, DO, Wan Lam, MD. C0131 - Pop Goes the Colon! An Unusual Case of Cecal Perforation, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.