Stephen G. Sinclair, DO1, David Y. Lo, MD, FACG2 1Mount Carmel Health Systems, Grove City, OH; 2Ohio Gastroenterology Group, Inc, and The Ohio State University College of Medicine, Columbus, OH
Introduction: Colonoscopy remains an effective modality for treatment of large polyps. Post-polypectomy surveillance is critical in evaluating for recurrence. The role of rectal endoscopic ultrasound (EUS) in post-polypectomy care remains unclear. In this case, we present a clinical scenario where rectal EUS was impactful.
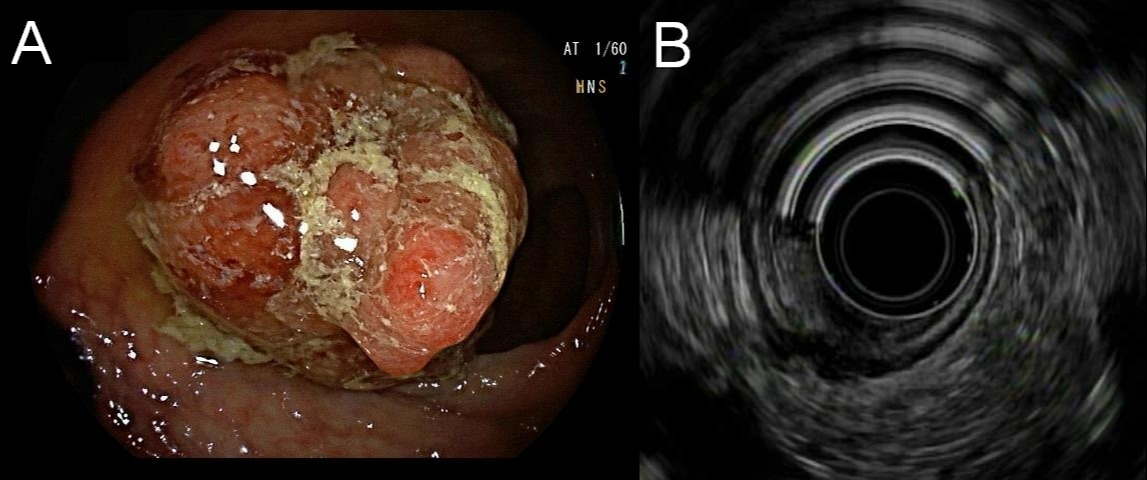
Case Description/Methods: A 50-year-old woman without a family history of colorectal cancer presented with a positive multitarget stool DNA test. Three months later, colonoscopy revealed a benign appearing 40mm rectosigmoid sessile polyp (A). Piecemeal polypectomy using hot snare over saline pillow was performed and the site was tattooed. Pathology showed a tubulovillous adenoma. She was then referred for a surveillance sigmoidoscopy.
Three months later, a recurrent 35mm sessile polyp was encountered at the previous tattoo site. The polyp was resected in a piecemeal fashion using saline injection lift with hot snare and hot biopsy avulsion. The polyp was difficult to remove due to the infiltrating tattoo and scarring from prior polypectomy. Pathology showed a villous adenoma.
Four months later, surveillance sigmoidoscopy revealed another recurrent 20mm polyp. Rectal EUS during the same session showed a 19mm x 10mm heterogeneous lesion with focal invasion into the muscularis propria (B). It was removed using saline injection lift, piecemeal resection with hot snare and cold forceps, and then ablated with argon plasma coagulation. Pathology again showed villous adenoma. Given the EUS findings, she was referred to surgical oncology. CT chest/abdomen/pelvis was negative for a mass and metastatic disease. CEA was only 0.99ng/mL. She then underwent lower anterior resection. Final pathology revealed well differentiated adenocarcinoma pT2 pN0 without lymph node metastasis. Surveillance colonoscopy less than a year later did not reveal any recurrent disease.
Discussion: Recurrence following piecemeal resection of sessile polyps is seen in up to 50% of patients in some studies. However, multiple recurrences are uncommon and warrant further investigation. Rectal EUS has been studied once previously for post resection of high-risk polyps and found to have only a slight incremental yield over white light endoscopy in the detection of cancer. In our case, rectal EUS did suggest underlying malignancy, which was confirmed on final surgical pathology. EUS in recurrent polyps is not well studied in the literature but may be a useful tool for the detection of underlying masses in these scenarios.
Figure: A. Rectosigmoid polyp. B. Heterogenous lesion with focal invasion into the muscularis propria.
Disclosures:
Stephen Sinclair indicated no relevant financial relationships.
David Lo indicated no relevant financial relationships.
Stephen G. Sinclair, DO1, David Y. Lo, MD, FACG2. C0190 - Endoscopic Ultrasound in the Diagnosis of Rectal Adenocarcinoma in a Recurrent Polyp, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.