Rosalind Franklin University of Medicine and Science McHenry, IL
Shirly Samuel, MD1, Arvin J. Mallari, MD1, Nicole Gentile, MD2 1Rosalind Franklin University of Medicine and Science, McHenry, IL; 2GI Partners of Illinois, McHenry, IL
Introduction: We present a case of acute esophageal necrosis (AEN) secondary to Trimethoprim-Sulfamethoxazole (TMP-SMX). There have been reports of other drugs implicated in the cause of AEN, however, to our knowledge this is the first case reporting AEN after TMP-SMX use.
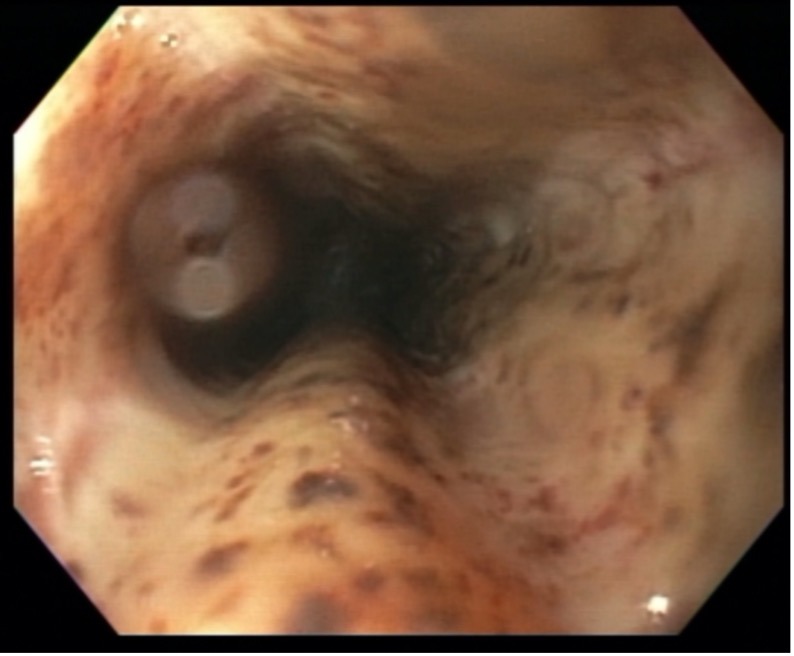
Case Description/Methods: A 70-year-old male with past medical history of type 2 diabetes mellitus, chronic kidney disease stage IV, hypertension, presented with epigastric pain, nausea, and vomiting. Four days prior he started taking TMP-SMX for a foot ulcer. Subsequently, he developed burning epigastric pain and multiple episodes of coffee ground emesis. On physical exam, he was tachycardic, pale, and had epigastric tenderness. Laboratory findings revealed white blood cell count of 19,100 /µL. He received a bolus of intravenous (IV) pantoprazole, followed by a continuous infusion. Esophagogastroduodenoscopy (EGD) revealed severe necrotic esophagitis with circumferential black eschar and severe friability, no linear tracking to suggest reflux at the beginning of the gastroesophageal junction, gastric mucosa was normal. Biopsy revealed ulcerative esophagitis with necrosis. Stains were negative for any viral or fungal organisms. Patient was discharged on pantoprazole and sucralfate.
Discussion: Acute esophageal necrosis (AEN) is a rare condition in which patients typically present with hematemesis or melena with endoscopy characterized by diffusely spread necrotizing lesions of the distal esophageal mucosa abruptly ending at the gastroesophageal junction. Several proposed mechanisms of AEN include hypoperfusion leading to ischemic injury, gastric acid damage, and suppressed protecting mechanisms [1]. AEN is more commonly found in older men in their seventh decade, with other co-morbidities such as diabetes, renal insufficiency, cardiac disease, hypertension, or history of alcohol abuse [3,4]. There are several drugs including NSAIDs, antihypertensive agents, cefazolin, terlipressin, clozapine to name a few which have caused AEN, however TMP-SMX has not been reported so far. Most of the drugs cause either a direct mucosal injury or induce changes in vascular perfusion [2]. Management of AEN includes discontinuing the offending agent and is mainly supportive care along with aggressive IV proton pump inhibitor (PPI) therapy initially until symptoms improve, then transitioning to oral PPI. Repeat EGD is recommended in one month to confirm healing of esophageal mucosa and to survey for strictures which is a possible complication [3].
Figure: Figure 1: EGD showing severe esophagitis with circumferential black eschar and severe friability.
Disclosures:
Shirly Samuel indicated no relevant financial relationships.
Arvin Mallari indicated no relevant financial relationships.
Nicole Gentile indicated no relevant financial relationships.
Shirly Samuel, MD1, Arvin J. Mallari, MD1, Nicole Gentile, MD2. C0238 - Acute Esophageal Necrosis From Trimethoprim-Sulfamethoxazole Use, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.


.jpg "Shirly Samuel, MD photo")