Stephen G. Sinclair, DO, Sohaib Hameed, DO Mount Carmel Health Systems, Grove City, OH
Introduction: Acute esophageal necrosis (AEN) is a rare syndrome also known as black esophagus. Aptly named, it is described as a circumferential, diffuse, black appearing esophageal mucosal lesion affecting variable lengths of the esophagus. Classically, the discoloration ends sharply at the gastroesophageal junction.
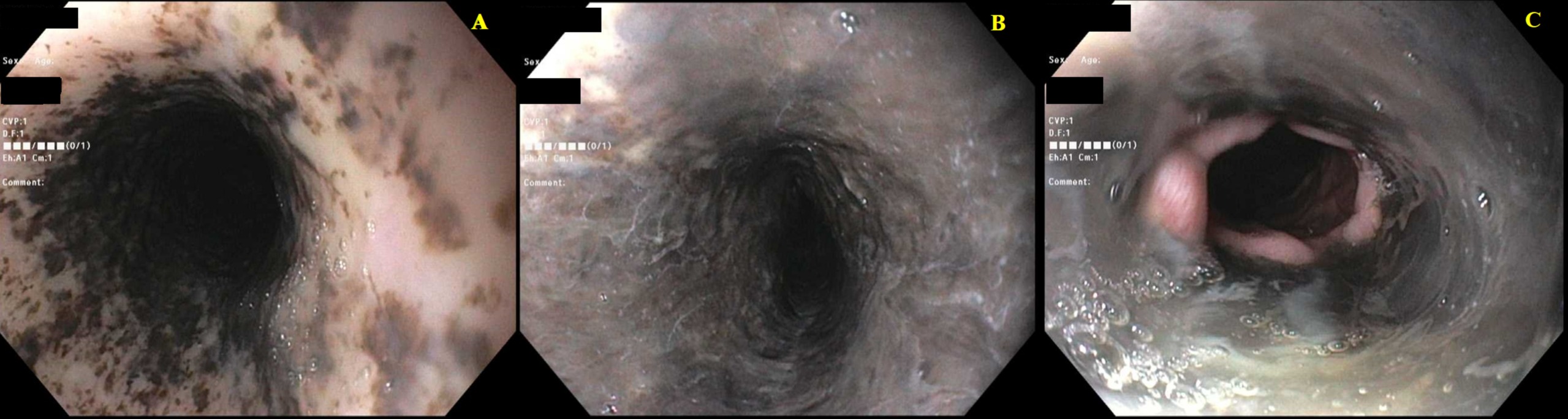
Case Description/Methods: A 50-year-old woman presented to the emergency department via ambulance for altered mental status. She had undergone 2 renal transplantations and was on chronic immunosuppression. She was intubated and treated for septic shock. CT scan demonstrated ureteral obstruction of her lone functioning transplant kidney with pyelonephritis and severe gastric distention suggestive of outlet obstruction. Nephrostomy tube was placed, and the patient was admitted to the critical care unit. Two days later, significant amount of coffee ground enteric contents was noted via nasogastric tube. Gastroenterology was consulted and twice daily intravenous proton pump inhibitor (PPI) was started. Urgent esophagogastroduodenoscopy was performed. Severe, circumferential black esophagitis was seen without ulceration. Intravenous PPI therapy and supportive care was continued. The patient was discharged 8 days from admission in stable condition with persisting odynophagia.
Discussion: This case represents the classical, two-insult presentation of AEN: septic shock and gastric outlet obstruction. Once diagnosis is established, careful surveillance is required. However, there are no established guidelines for surveillance. The most important and life-threatening complication is perforation and should be suspected if rapid clinical worsening is seen. Per expert opinion, PPI therapy should be transitioned to oral therapy once improvement is noted and continued until repeat endoscopy in approximately 8 weeks. As of 2006, there were 88 cases documented in medical literature. AEN is thought to require two insults due to the significant collateral and segmental blood supply of the esophagus. First, global hypoperfusion is expected. Second, profound mucosal injury from reflux of gastric contents. Treatment includes managing the underlying medical conditions, supportive care, and PPI therapy. Complications following AEN are strictures, abscesses, and perforation. Associated mortality is approximately 30%. This is likely due to the underlying medical conditions that cause AEN. Awareness and understanding of the condition and its complications is important to manage and surveil survivors appropriately.
Figure: A- Upper third of the esophagus. B- Middle third of the esophagus C- Lower esophageal sphincter
Disclosures:
Stephen Sinclair indicated no relevant financial relationships.
Sohaib Hameed indicated no relevant financial relationships.
Stephen G. Sinclair, DO, Sohaib Hameed, DO. C0263 - A Classic Case of Black Esophagus, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.