Lincoln Medical and Mental Health Center Bronx, NY
Ebehiwele Ebhohon, MD1, Abdultawab Shaka, MBBS2, Pius Ojemolon, MBBS3, Robert Kwei-Nsoro, MD4, Hisham Laswi, MD5, Hafeez Shaka, MBBS5 1Lincoln Medical Center, Bronx, NY; 2John H. Stroger, Jr. Hospital of Cook County, Chicago, IL; 3John H. Stroger Jr. Hospital of Cook County, Chicago, IL; 4John H. Stroger, Jr Hospital of Cook County, Chicago, IL; 5John H. Stroger, Jr. Hospital of Cook County, Chicago, IL
Introduction: Functional dyspepsia (FD), a diagnosis of exclusion, has a 10–20% prevalence(1,2). The pathophysiology is unclear, often multifactorial, and involves treatment with a detailed education about its benign nature. Tricyclic antidepressants and psychotherapy are warranted if functional dyspepsia (FD) is refractory or severe (1). Functional dyspepsia (FD) can present with postprandial distress (70% of FD cases) or epigastric pain syndrome (30% of FD cases) (3). FD can decrease quality of life and place a significant cost burden on healthcare services. Our study sought to determine the rate and reasons for 30-day all-cause readmissions for FD to help identify potentially modifiable factors and decrease the burden of readmissions.
Methods: From the NRD, we identified all adults discharged with a principal diagnosis of FD after hospitalization from 2016 to 2019. Then, we identified any readmission of the same patient within 30-days for FD, excluding elective and traumatic encounters. Outcomes assessed included 30-day all-cause readmissions, top principal diagnosis for the readmitted patients, comparison of mortality, length of stay (LOS), and total hospital charges (THC) following readmission.
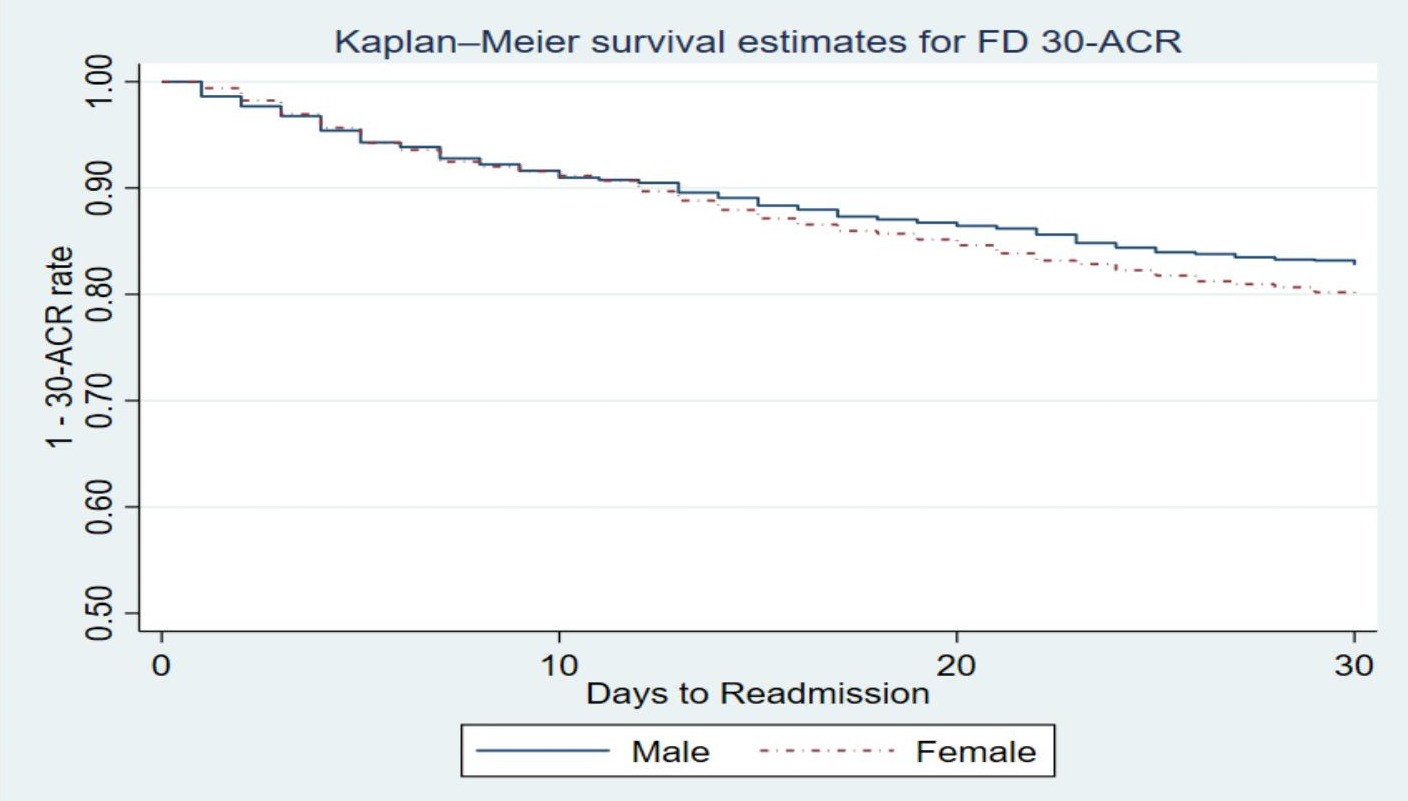
Results: 4 917 patients with FD during index admissions were identified. The 30-day all-cause readmission rate was 19.3%. The Kaplan-Meier curve for 30-day all-cause readmissions was split by sex (Fig.1). There was no significant difference in age and sex distribution between patients with initial hospitalizations and those with readmissions. The most common reasons for readmissions in patients with FD were gastroparesis (5.9%), FD (5.8%), sepsis unspecified (5.2%), unspecified nausea and vomiting (3.1%), unspecified abdominal pain (2.1%), and acute renal failure (2.0%). Readmission was associated with higher odds of mortality (2.8% vs. < 0.01%, p< 0.001), longer LOS (6.0 vs. 5.0 days, p< 0.001), and higher THC. Over the period, readmissions for FD accounted for a cumulative 5.694 days of hospitalization, costing over $14 million.
Discussion: 1 in 4 patients was readmitted with FD within 30 days. Gastroparesis contributed more to readmissions than a primary diagnosis of FD. Higher rates of poorer outcomes were found with 30-days readmissions. Cohort studies are needed to validate these results.
Figure: Fig. 1: Survival estimates for 30-day all-cause readmissions in male and Female patients with functional dyspepsia
Disclosures:
Ebehiwele Ebhohon indicated no relevant financial relationships.
Abdultawab Shaka indicated no relevant financial relationships.
Pius Ojemolon indicated no relevant financial relationships.
Robert Kwei-Nsoro indicated no relevant financial relationships.
Hisham Laswi indicated no relevant financial relationships.
Hafeez Shaka indicated no relevant financial relationships.
Ebehiwele Ebhohon, MD1, Abdultawab Shaka, MBBS2, Pius Ojemolon, MBBS3, Robert Kwei-Nsoro, MD4, Hisham Laswi, MD5, Hafeez Shaka, MBBS5. C0269 - Rate and Reasons for Non-Elective 30-Day Readmissions for Functional Dyspepsia in the U.S., ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.