Minji Seok, BA1, Krutika Lakhoo, MD2, Anna M. Lipowska, MD1 1University of Illinois at Chicago, Chicago, IL; 2University of Illinois, Chicago, IL
Introduction: Cecal bascules are the rarest variant of cecal volvulus that involve upward folding of the cecum, without axial twisting or sigmoid involvement. We present a case in which a patient with a hepatic flexure obstruction from extrinsic compression masqueraded as a cecal bascule on imaging.
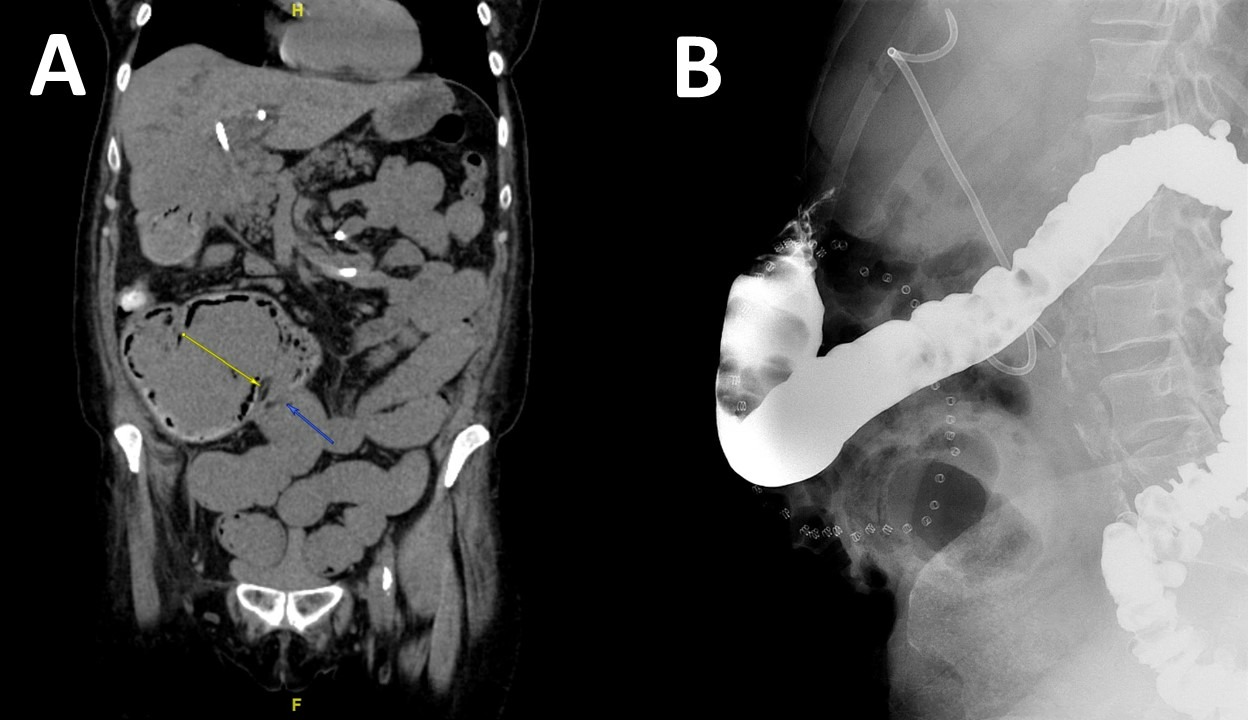
Case Description/Methods: A 66-year-old woman with history of stroke, hypertension, recent obstructive cholestasis due to choledocholithiasis requiring biliary stent placement, presented with 3 days of right sided abdominal pain, 15lb weight loss and 3 weeks of constipation with thin stools. Computed Tomography (CT) revealed dilated loops of distal small bowel and cecum that folded anteriorly and superiorly with extensive pneumatosis (Figure 1A), consistent with cecal bascule (type III cecal volvulus). The ascending colon was dilated up to a decompressed hepatic flexure, where nonspecific bowel wall thickening was visualized. She had a normal colonoscopy a few months prior. The patient was initially managed conservatively, however a lower gastrointestinal series showed persistent obstruction at the hepatic flexure with bird-beak appearance (Figure 1B). She underwent an exploratory laparotomy that discovered a mass in the right upper quadrant involving the gallbladder and liver, causing extrinsic compression of the hepatic flexure and numerous omental nodules. Biopsies confirmed metastatic cholangiocarcinoma. The patient began evaluation for cancer staging, but ultimately passed one month after diagnosis.
Discussion: The development of a cecal bascule is usually attributed to an abnormally mobile cecum due to improper development and insufficient fixation of the mesentery to the posterior parietal peritoneum. A mobile cecum may also be acquired in pregnancy due to enlargement of the uterus, or after abdominal surgery such as open appendectomies which require extensive division of peritoneal attachments to the cecum. Clinical presentation can be variable with abdominal pain, distention and nausea being most common symptoms and ranging to an acute abdomen and perforation. Diagnosis of type III cecal volvulus requires CT imaging confirming a distended cecum lying anterior to ascending colon. Treatment generally involves surgical resection of the affected bowel as colonoscopic detorsion may lead to recurrence. This is a unique case of an extrinsic malignant obstruction causing a cecal bascule, highlighting the importance of a comprehensive evaluation for underlying etiologies.
Figure: Figure 1A: Cecal bascule with extensive pneumatosis on CT. Figure 1B: Lower gastrointestinal series showing obstruction at hepatic flexure with bird-beak appearance.
Disclosures:
Minji Seok indicated no relevant financial relationships.
Krutika Lakhoo indicated no relevant financial relationships.
Anna Lipowska indicated no relevant financial relationships.
Minji Seok, BA1, Krutika Lakhoo, MD2, Anna M. Lipowska, MD1. B0138 - Extrinsic Compression of the Hepatic Flexure from Metastatic Cholangiocarcinoma Masquerading as Cecal Bascule, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.