Texas Tech Health Sciences Center, Paul L. Foster School of Medicine El Paso, TX
Nikita Lobo, MS1, Jenson Erapuram, MD2, Abhizith Deoker, MD2 1Texas Tech Health Sciences Center, Paul L. Foster School of Medicine, El Paso, TX; 2Texas Tech Health Sciences Center El Paso, El Paso, TX
Introduction: Pseudomyxoma peritonei (PMP) is a rare disorder characterized by the accumulation of gelatinous material within the abdomen and pelvis. While usually appendiceal in origin, it can be seen with mucinous tumors arising from the ovary, GI tract, urachus, and pancreas. We describe a case of pancreatic adenocarcinoma diagnosed due to the clinical syndrome precipitated by pseudomyxoma peritonei.
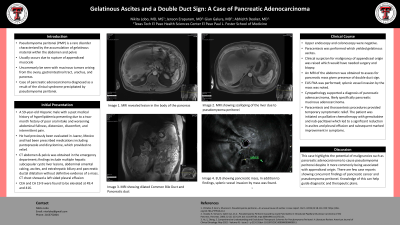
Case Description/Methods: A 59-year-old Hispanic male presented to the hospital for evaluation due to a 2 month history of poor oral intake and worsening abdominal fullness, distension, discomfort, and intermittent pain. The patient reported one prior hospitalization for pancreatitis of unclear etiology, 3 years ago. A CT abdomen & pelvis was obtained; findings reported include multiple hepatic subcapsular cystic liver lesions, abdominal omental caking, ascites, and extrahepatic biliary and pancreatic ductal dilatation without definitive evidence of a mass. CEA and CA 19-9 were found to be elevated at 49.4 and 416 respectively. CT chest revealed a left-sided pleural effusion. Upper endoscopy and colonoscopy were negative. Paracentesis yielded gelatinous ascites. Clinical suspicion for appendiceal malignancy was raised which required surgical exploration and biopsy to confirm. An MRI of the abdomen was obtained to assess for pancreatic mass given presence of double duct sign. MRI revealed 2.2 x 2.7 x 5 cm lesion in the body of the pancreas, pseudomyxoma peritonei with scalloping of the liver and extension into the right posterior mediastinum via the esophageal hiatus, metastatic deposits in the porta hepatis and peritoneal carcinomatosis. No apparent abnormality in the appendix was observed. EUS FNA was performed; splenic vessel invasion by the mass was noted. Cytopathology supported a diagnosis of pancreatic adenocarcinoma. The patient was initiated on palliative chemotherapy with gemcitabine and nab-paclitaxel which led to a significant reduction in ascites and pleural effusion and improvement in symptoms.
Discussion: This case highlights the potential of malignancies such as pancreatic adenocarcinoma to cause pseudomyxoma peritonei despite it more commonly being associated with appendiceal origin. Knowledge of this can help guide diagnostic and therapeutic plans.
Disclosures:
Nikita Lobo indicated no relevant financial relationships.
Jenson Erapuram indicated no relevant financial relationships.
Abhizith Deoker indicated no relevant financial relationships.
Nikita Lobo, MS1, Jenson Erapuram, MD2, Abhizith Deoker, MD2. A0065 - Gelatinous Ascites and a Double Duct Sign: A Case of Pancreatic Adenocarcinoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.