Tenzin Tseky, DO, Grace E. Yi, DO, Vidhya Reddy, MD, Troyce Fortune, DO, Nedal Darwish, MD, Dayakar Reddy, MD Arnot Ogden Medical Center, Elmira, NY
Introduction: Afferent limb syndrome (ALS) is a rare complication of gastrojejunostomy, where the excluded segment carrying digestive juices termed the afferent limb is obstructed distally from varying etiologies. We present a case of pancreatic mass which presented as ALS in a female with a history of Roux-en-Y gastric bypass (RYGB) managed via percutaneous gastrostomy tube (G-Tube) decompression.
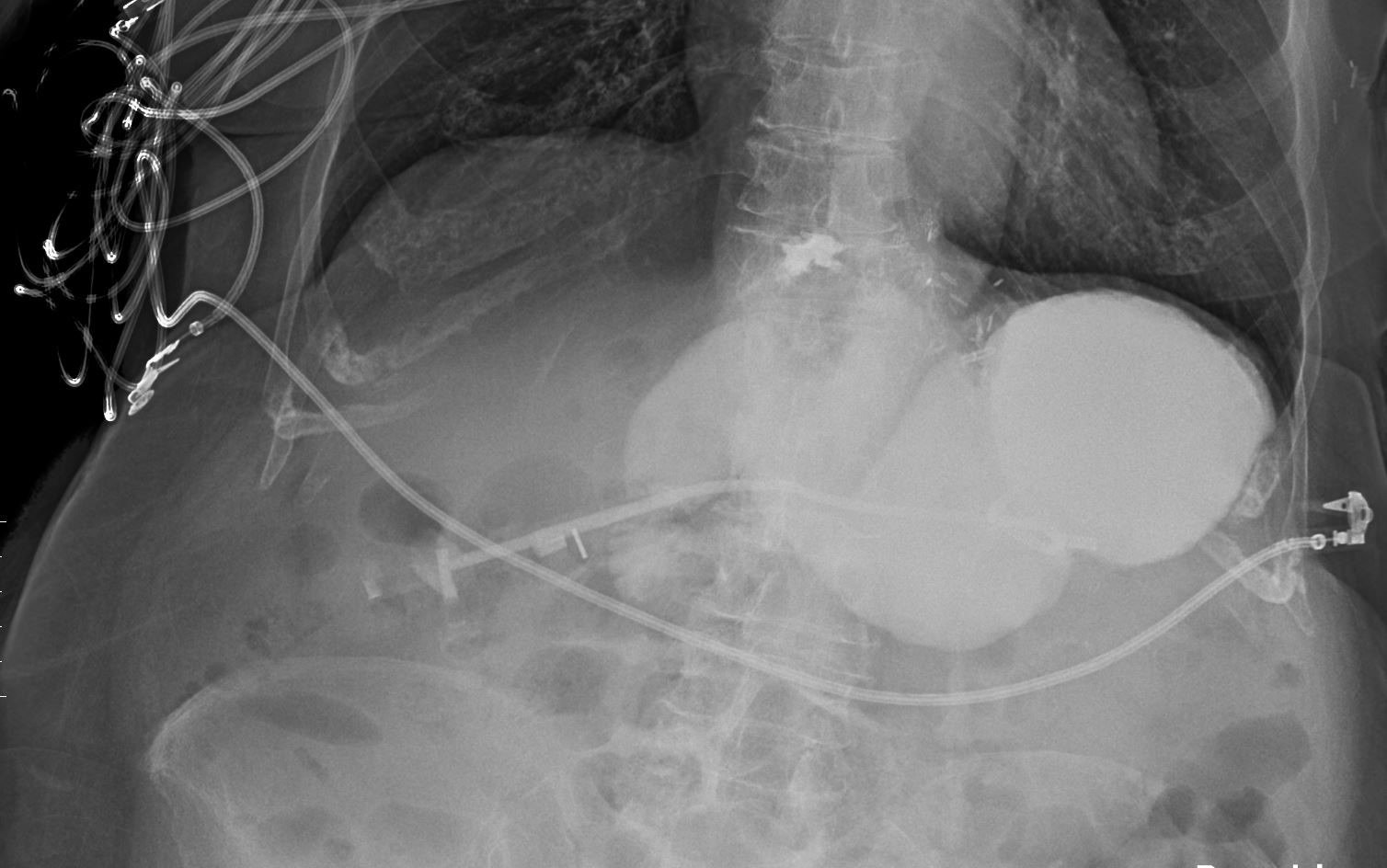
Case Description/Methods: A 75-year-old female with a remote history of RYGB presented to the emergency department (ED) due to few days of nausea and dry heaves. Evaluation revealed a hemodynamically stable patient with abdominal distention, and grossly benign laboratory values. Computed tomography (CT) abdomen indicated obstruction with fluid distention of the gastric remnant to the level of the third portion of the duodenum. Supportive care was initiated. General surgery assessed this to be ALS, and recommended medical admission, bowel rest, and G-Tube decompression. Ultrasound-guided percutaneous G-Tube was inserted at the dilated limb, which instantly drained a liter of bilious fluid, and continued for a few more days with exceptional clinical improvement and return of bowel function. Upper GI series was obtained using G-Tube catheter as insertion site for contrast which showed it persisting in the afferent limb for almost 6 hours as in Figure 1. CT abdomen with intravenous contrast confirmed 2.1x1.6 cm soft tissue lesion involving the uncinate process. Arrangements were made for transfer to tertiary center for surgical oncology evaluation.
Discussion: ALS is a rare complication of gastrojejunostomy due to distal obstruction of the afferent limb leading to accumulation of digestive secretions here while the alimentary limb remains patent. Etiology includes adhesions, stenosis from marginal ulceration, cancer recurrence, and enteroliths. CT finding of dilated afferent limb is diagnostic. Management involves consideration of etiology, site, and functional status. In malignant ALS, management targets primarily palliative treatment and secondarily surgery with curative intent. Key points from the case are: While ALS most commonly follows Billroth II, it can occur in RYGB; Decompression via G-tube placed at the dilated limb proximal to obstruction serves as a palliative measure prior to definitive surgery; While most malignant ALS cases involve recurrence, this mass was uncovered via ALS; While conventional management of malignant ALS was surgical, percutaneous and endoscopic methods are increasingly being employed.
Figure: Figure 1: Upper GI series with contrast injected via the catheter of the percutaneous gastrostomy tube demonstrates persistent contrast in the excluded portion of the reconstruction including the gastric remnant and proximal duodenum at 5 hours and 40 minutes.
Disclosures:
Tenzin Tseky indicated no relevant financial relationships.
Grace Yi indicated no relevant financial relationships.
Vidhya Reddy indicated no relevant financial relationships.
Troyce Fortune indicated no relevant financial relationships.
Nedal Darwish indicated no relevant financial relationships.
Dayakar Reddy indicated no relevant financial relationships.
Tenzin Tseky, DO, Grace E. Yi, DO, Vidhya Reddy, MD, Troyce Fortune, DO, Nedal Darwish, MD, Dayakar Reddy, MD. A0063 - Pancreatic Neoplasm Presenting as Afferent Limb Syndrome in a Patient With a Remote History of Roux-en-Y Gastric Bypass, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.