FMH College of Medicine & Dentistry Lahore, Punjab, Pakistan
Ali Waqar Chaudhry, MD1, Sadaf Raoof, MD2, Syed Hamaad Rahman, DO3, Nihal Ijaz Khan, MBBS4, Abdul Arham, MBBS5, Abu Hurairah, MD2, Gurdeep Singh, DO2 1FMH College of Medicine & Dentistry, Lahore, Punjab, Pakistan; 2AdventHealth Orlando, Orlando, FL; 3Methodist Dallas Medical Center, Dallas, TX; 4Allama Iqbal Medical College, Sarnia, ON, Canada; 5Allama Iqbal Medical College, Mississauga, ON, Canada
Introduction: Goblet Cell Adenocarcinomas (GCAs) are a very rare subtype of appendiceal tumors, with an estimated incidence of 1 per 2 million people. They are not only rare but also unique in terms of their origin. Whereas most cancers arise from one cell line, goblet cell adenocarcinomas are a hybrid of neuroendocrine cells and epithelial cells. The aim of this abstract is to provide an overview of this unique clinical entity.
Case Description/Methods: We present a case of a 62-year-old female with past medical history of hypertension, diabetes mellitus and hyperlipidemia who presented to the ED with a one day history of right lower quadrant abdominal pain that had migrated from the periumbilical area, associated with non-bloody vomiting. On arrival, she was stable and her physical examination was significant for tenderness in the right lower quadrant and a positive Rovsing and obturator sign. Labs were remarkable for leukocytosis with left shift. CT scan of the abdomen was done which revealed an inflamed appendix and subsequently patient was taken for a laparoscopic appendectomy. Pathology of the surgical specimen revealed a well differentiated T1NxMx GCA with negative margins and no lymphovascular or perineural invasion. A decision was made to proceed with a right hemicolectomy for the purpose of staging and treatment. Pathology sent after right hemicolectomy revealed no residual GCA with 21 lymph nodes negative for metastasis and negative surgical margins.
Discussion: First described in 1969, GCAs mostly occur in the 5th and 6th decade of life with equal prevalence in both genders. GCAs most commonly present as acute appendicitis but can also present with abdominal pain associated with abdominal mass and weight loss. They can metastasize to the peritoneum, omentum, abdominal wall, and ovaries. Majority of GCAs are diagnosed incidentally on pathological examination of inflamed appendix after appendectomy. The mainstay of treatment is surgical resection with the addition of adjuvant chemotherapy for node-positive (stage III) disease or higher. Due to the rarity of this condition, there is lack of consensus regarding the extent of surgical resection. For stage I disease appendectomy alone maybe sufficient, but higher stages may require hemicolectomy. Prognosis depends on the grade and stage at diagnosis, with one retrospective analysis reporting 5-year survival rates of 100%, 76%, 22%, and 14% for stages I, II, III, and IV, respectively.
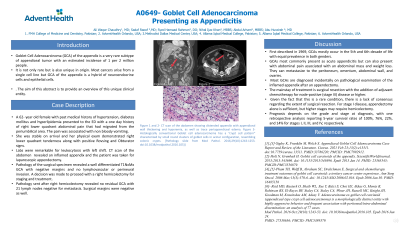
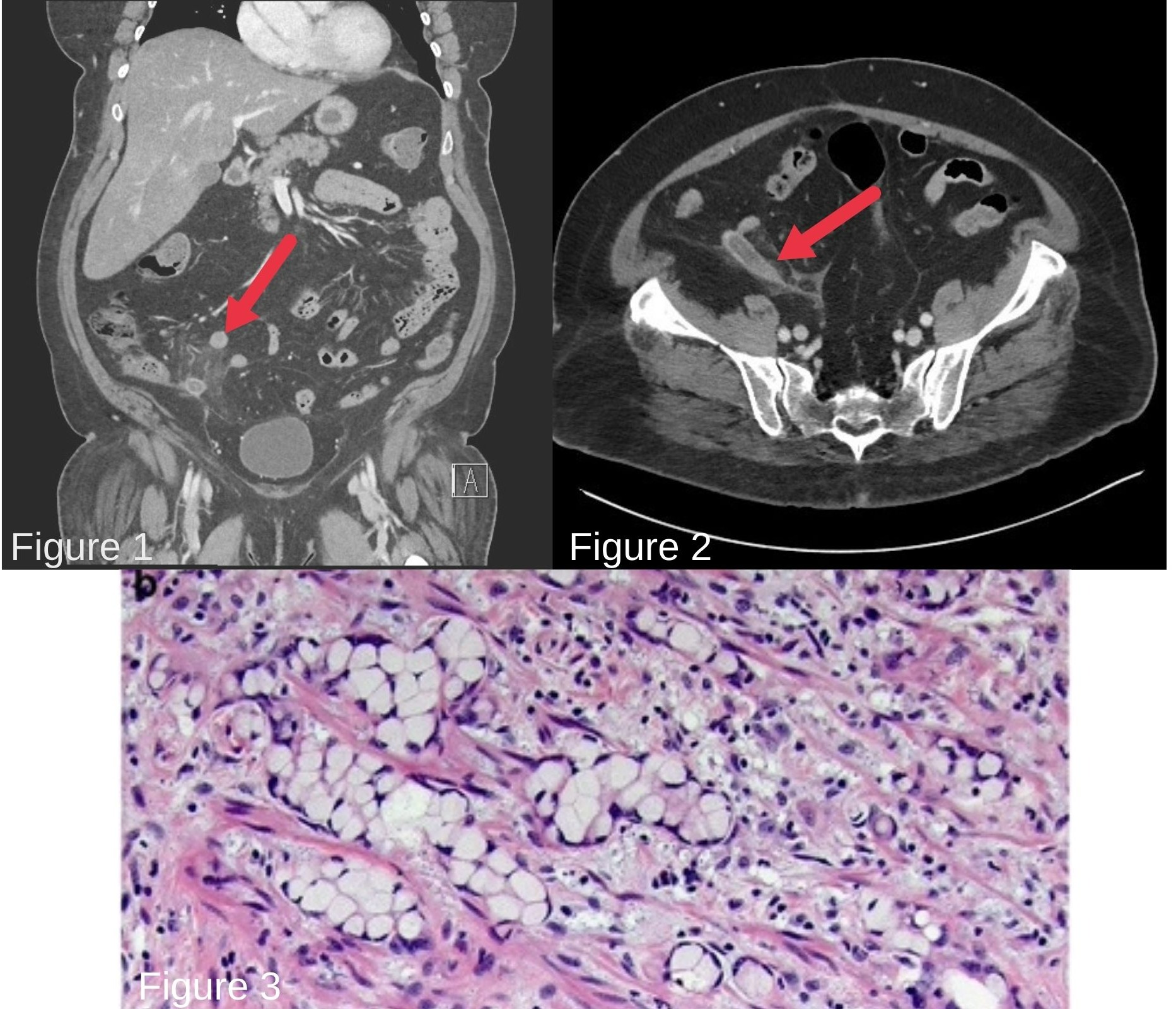
Figure: Figure 1 and 2- CT scan of the abdomen showing distended appendix with appendiceal wall thickening and hyperemia, as well as trace periappendiceal edema. Figure 3- Histologically conventional Goblet cell adenocarcinoma has a “crypt cell pattern” characterized by small round clusters of goblet cells in acinar configuration, resembling colonic crypts. [Pathology slide from Mod Pathol. 2016;29(10):1243-1253. doi:10.1038/modpathol.2016.105)]
Disclosures:
Ali Waqar Chaudhry indicated no relevant financial relationships.
Sadaf Raoof indicated no relevant financial relationships.
Syed Hamaad Rahman indicated no relevant financial relationships.
Nihal Ijaz Khan indicated no relevant financial relationships.
Abdul Arham indicated no relevant financial relationships.
Abu Hurairah indicated no relevant financial relationships.
Gurdeep Singh indicated no relevant financial relationships.
Ali Waqar Chaudhry, MD1, Sadaf Raoof, MD2, Syed Hamaad Rahman, DO3, Nihal Ijaz Khan, MBBS4, Abdul Arham, MBBS5, Abu Hurairah, MD2, Gurdeep Singh, DO2. A0649 - Goblet Cell Adenocarcinoma Presenting as Appendicitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.