San Antonio Military Medical Center Fort Sam Houston, TX
Christina Awad, MD, Ryan Cho, MD, John Quiles, MD San Antonio Military Medical Center, Fort Sam Houston, TX
Introduction: Duodenal duplication cyst (DDC) is a rare congenital anomaly that often presents in the neonatal period with presentations later in life less common. Duplication cysts can develop anywhere from the mouth to the anus with only 4-12% are located in the duodenum. DDC is an uncommon cause of acute pancreatitis but the diagnosis is difficult to make in adults because the symptoms are non-specific. We present a case of diagnostic dilemma of a 53 years old female patient with recurrent acute pancreatitis (RAP), attributed to DDC.
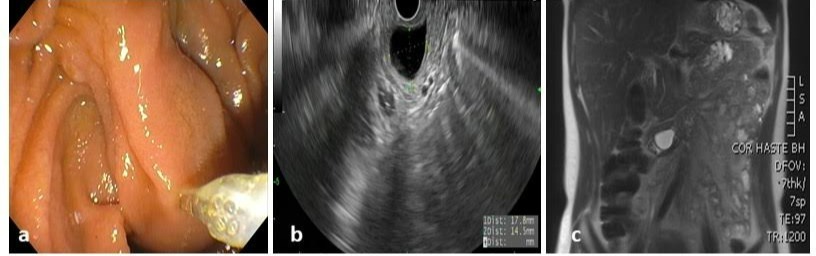
Case Description/Methods: Her first index episode of pancreatitis was 12 years prior to her presentation. Patient was found to have a large cyst in the 2nd portion of the duodenum that appeared to be separate from the biliary tree and pancreas on EGD (Figure 1a), EUS (Figure 1b) and MRI (figure 1c), abutting the major papilla. The initial EUS showed a 20 mm x 13.4 mm anechoic cyst with layering and debris seen in the cavity. Aspiration of the cyst was performing, returning with elevated CEA at 817 ng/mL. No features of chronic pancreatitis were seen. Given elevated CEA, there was a concern for mucinous cyst, prompting a repeat EUS. EUS guided biopsy of the internal cyst wall was performed and histology was consistent with small bowel suggestive of a duplication cyst.
Discussion: Our patient presented with recurrent episodes of pancreatitis that could be explained by the intermittent occlusion of the pancreatic duct by debris and sludge found within the cyst. The elevated CEA and inconclusive radiographic results initially suggested possible mucinous cyst, presenting a diagnostic dilemma. Therefore, EUS guided biopsies were essential to confirm the diagnosis and allowing for further endoscopic management. The presence of a smooth muscle coat is absolutely essential for the diagnosis of a duplication cyst which was the case for our patient. DDC are covered both inside and outside by duodenal mucosa containing a distinct layer of smooth muscle. Given its malignancy potential, resection of these cysts is indicated. Endoscopic resection is minimally invasive and has been proposed as an alternative to surgery in selected patients especially given the close proximity of major papilla. Resection techniques using standard polypectomy, or large incision of the roof of the duplication cyst has been discussed in the literature. In our case, endoloop was applied around the base of the cyst, leading to strangulation and necrosis for obliteration of the cyst.
Figure: Figure 1a shows a large cyst in the 2nd portion of the duodenum that appeared to be separate from the biliary tree and pancreas on EGD abutting the major papilla, Figure 1b shows the cysts on EUS and figure 1c shows the cyst on MRI.
Disclosures:
Christina Awad indicated no relevant financial relationships.
Ryan Cho indicated no relevant financial relationships.
John Quiles indicated no relevant financial relationships.
Christina Awad, MD, Ryan Cho, MD, John Quiles, MD. B0470 - Diagnostic Dilemma: Utilizing Endoscopic Ultrasound (EUS) Guided Biopsy to Assist With the Diagnosis of the Duodenal Duplication Cyst, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.