Scott N. Berger, MD, Juan D. Gomez Cifuentes, MD, Tara Keihanian, MD, Wasif Abidi, MD, PhD, Kalpesh K. Patel, MD Baylor College of Medicine, Houston, TX
Introduction: Accessing excluded parts of the GI tract via lumen-apposing metallic stent (LAMS) has opened a new horizon of possibilities for biliary and luminal interventions in patients with altered anatomy including Roux-en-Y gastric bypass (RYGB). LAMS is routinely placed for biliary intervention in patients with RYGB, however data is lacking to demonstrate its feasibility for bowel decompression. Here, we present a case of a percutaneous endoscopic gastrostomy (PEG) tube placement in the bypassed stomach using LAMS.
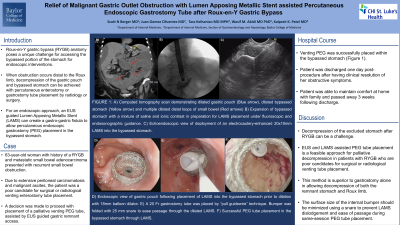
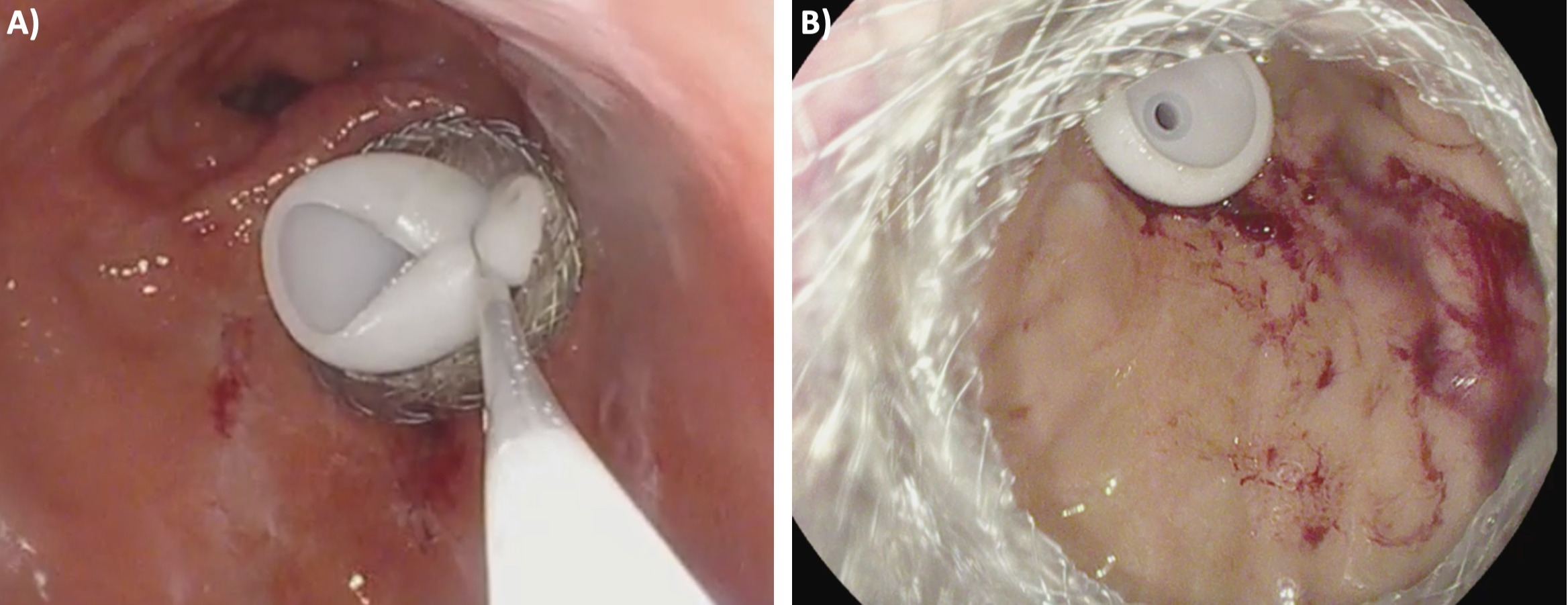
Case Description/Methods: A 63-year-old woman with a history of a lap-band converted to RYGB and metastatic small bowel adenocarcinoma on palliative chemotherapy presented with recurrent small bowel obstruction. Due to her extensive peritoneal carcinomatosis and malignant ascites, she was a poor candidate for surgical or radiological enterostomy tube placement. A decision was therefore made to proceed with a palliative LAMS assisted PEG tube placement. Under endoscopic ultrasound guidance, the bypassed stomach was punctured with a 19-gauge fine needle aspiration Slimline needle. A mixture of iodinated contrast with normal saline was injected, resulting in expansion of the bypassed stomach under fluoroscopic guidance. Following this, an electrocautery enhanced AXIOS delivery catheter was used to puncture and deploy a 20 mm x 10 mm LAMS into the bypassed stomach. The AXIOS was then dilated with a through-the-scope balloon dilator to a maximum diameter of 18mm under fluoroscopy. The endoscope was passed through the stent and the bypassed stomach was insufflated with carbon dioxide to oppose the gastric and abdominal walls. A 20Fr gastrostomy tube was then placed using the “pull guidewire” technique in the distal gastric body. A 25mm snare was used to grasp the bumper in order to minimize the surface size for ease of passage through the AXIOS stent. There was no immediate adverse event and the patient was successfully discharged one day post procedure after clinical resolution of her obstructive symptoms.
Discussion: The venting tube is usually placed radiologically or surgically within the alimentary limb of the jejunum in patients with RYGB. However, in certain patients with obstruction distal to the jejuno-jejunal anastomosis or within the biliopancreatic limb, decompression of the excluded stomach is required. This case illustrates the feasibility of an EUS assisted venting PEG tube in a patient with gastric bypass anatomy.
Figure: FIGURE 1: A) Minimizing bumper surface size with a snare for ease of passage through the AXIOS stent. B) Successful placement of percutaneous gastronomy placement through an AXIOS stent
Disclosures:
Scott Berger indicated no relevant financial relationships.
Juan Gomez Cifuentes indicated no relevant financial relationships.
Tara Keihanian indicated no relevant financial relationships.
Wasif Abidi: Ambu USA – Consultant. Apollo Endosurgery – Consultant. ConMEd – Consultant. GI dynamics – Grant/Research Support.
Kalpesh Patel: Boston Scientific – Consultant.
Scott N. Berger, MD, Juan D. Gomez Cifuentes, MD, Tara Keihanian, MD, Wasif Abidi, MD, PhD, Kalpesh K. Patel, MD. C0468 - Relief of Malignant Gastric Outlet Obstruction With Lumen Apposing Metallic Stent-Assisted Percutaneous Endoscopic Gastrostomy Tube After Roux-en-Y Gastric Bypass, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.