University of Colorado Anschutz Medical Center Aurora, CO
Abigail Braun, MD, Alexander Hayden, MD, Arun Kannappan, MD University of Colorado Anschutz Medical Center, Aurora, CO
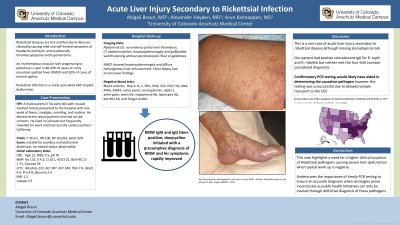
Introduction: The differential diagnosis of acute liver injury (ALI) is broad and includes toxins, inflammatory, vascular, and infectious etiologies. Most infectious ALI cases in the US stem from viral hepatitis, though rarer causes exist. In this case, workup of ALI revealed rickettsial-induced acute liver injury, which is a rare presentation of rickettsial disease.
Case Description/Methods: A man with no past medical history presented to the Emergency Department with one week of fevers, myalgias, vomiting, and malaise. He was febrile, tachycardic, hypotensive, and jaundiced. No rash was identified. He lived in Colorado and had recently traveled to Southern California. Laboratory workup revealed platelets of 70,000 , AST 232 U/L, ALT 287 U/L, alkaline phosphatase 216 U/L, and total bilirubin 7.6 mg/dl. His INR was elevated to 1.2. Urine toxicology screens were negative. Abdominal imaging revealed hepatosplenomegaly. He was started on broad spectrum antibiotics due to concern for severe sepsis. Hepatitis serologies, EBV, CMV, VZV, HSV, and HIV were negative. Testing for autoimmune etiologies, Wilson’s disease, and alpha-1 antitrypsin were also negative. MRCP had no ductal obstruction and liver biopsy was inconclusive. Additional studies were notable for elevated Rocky Mountain Spotted Fever and typhus antibody titers concerning for rickettsial infection. He was given doxycycline and rapidly improved with normalization of liver enzymes. Repeat convalescent serologies remained elevated for both Rickettsia species and were inconclusive as to which organism was the causative pathogen. CDC confirmatory testing was sent but the sample was unable to be processed due to the amount of time between test collection and arrival at the laboratory.
Discussion: Rickettsial diseases classically cause rash, headache, fever, thrombocytopenia, and hyponatremia. While mild transaminase elevations accompany infection, there are few cases of rickettsial species causing acute liver injury.
This case highlights the need for clinical suspicion of rickettsial pathogens causing severe liver dysfunction when standard evaluation is negative, even in instances where rash and travel exposure are absent. When rickettsial infection is suspected, antibiotics are often begun while awaiting laboratory testing. However, serologic testing for rickettsial pathogens is often inconclusive and timely PCR based evaluation through the CDC is required for a definitive diagnosis.
Disclosures:
Abigail Braun indicated no relevant financial relationships.
Alexander Hayden indicated no relevant financial relationships.
Arun Kannappan indicated no relevant financial relationships.
Abigail Braun, MD, Alexander Hayden, MD, Arun Kannappan, MD. A0531 - Acute Liver Injury Secondary to Rickettsial Infection, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.