Fady Banno, MD, MSc, Brandon Wiggins, DO, MPH, Kyle Knight, DO, Kanksha Peddi, MD, Nathan Landesman, DO Ascension Genesys Hospital, Grand Blanc, MI
Introduction: Primary adenocarcinoma of the appendix is an uncommon malignancy of the gastrointestinal tract. It was first described in 1882 and constitutes around 0.12 to 2.6 cases per one million people per year. In addition, signet-ring cell carcinoma of the appendix is extremely rare, it constitutes approximately 4% of all primary appendiceal neoplasms. There are few reported cases of primary signet cell appendiceal carcinoma. In this present report, we describe a rare case of primary signet ring cell carcinoma of the appendix with omental metastases in an 81-year-old male who underwent laparoscopic appendectomy.
Case Description/Methods: We present a case of an 81-year-old male who had prior negative esophagogastroduodenoscopy (EGD) and colonoscopy in 2017 who presented to an urgent care in January 2021 with abdominal pain. Lab work was unremarkable, and the patient was sent home with instructions to visit the emergency department (ED) if he experienced fever, increased abdominal pain, or blood in the stool. Patient presented to the emergency department with increased abdominal pain in April 2021, and Computed Tomography (CT) scan of abdomen and pelvis with intravenous contrast showed a cystic appendiceal lesion with right peritoneal nodularity suspicious for peritoneal carcinomatosis. Therefore, the patient underwent appendectomy the following day revealing poorly differentiated, high-grade appendiceal adenocarcinoma with signet ring features, pT4a disease
Patient had a diagnostic laparoscopy in June 2021 and was found to have diffuse peritoneal carcinomatosis. Multiple biopsies were obtained and came back positive with high-grade mucinous adenocarcinoma with signet ring features. Patient agreed to pursue systemic chemotherapy. He was initiated on Capecitabine (Xeloda) 2000 mg tab PO, twice daily for 14 days and off for 7 days. Bevacizumab (Avastin) 7.5 mg IV infusion every 3 weeks.
Discussion: Patients with appendiceal neoplasms may have vague lower abdominal pain but are usually asymptomatic with incidental diagnosis on imaging or appendectomy. Signet ring adenocarcinoma of the appendix typically secretes mucin leading to metastasis throughout the peritoneum and eventual obstruction. Treatment is based on stage and histology. Surgical resection and peritoneal debulking is possible. High-grade tumors require further prospective trials to evaluate treatment, but treatment options include surgical management, HIPEC, and systemic chemotherapy.
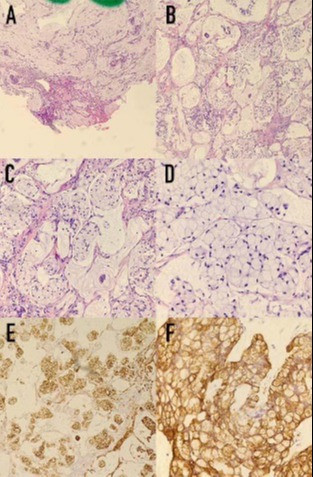
Figure: Histologic examination showing a signet cell carcinoma of the appendix infiltrating the peritoneum and diaphragm. (A) right lower quadrant peritoneum biopsy, (H&E stain 100x): High grade mucinous carcinoma peritonei with signet ring cells. Pool of mucin with a cluster of epithelium that shows signs of metastatic carcinoma (enlarged nuclei, atypia, pleomorphic changes). (B, C, and D) Right diaphragm peritoneum biopsy. High grade mucinous carcinoma peritonei with signet ring cells. Image B at 100x, C at 200x, and D at 400x. (E & F) immunohistochemical cytokeratin stain (AE1/AE3) shows strong positivity of high grade carcinoma. E at 100x, and F at 400x.
Disclosures:
Fady Banno indicated no relevant financial relationships.
Brandon Wiggins indicated no relevant financial relationships.
Kyle Knight indicated no relevant financial relationships.
Kanksha Peddi indicated no relevant financial relationships.