Sarah Elrod, DO1, Kyle Marrache, DO1, Zulfiqar Arif, MD2 1Abington-Jefferson Hospital, Abington, PA; 2Abington Plaza Medical Association, Warrington, PA
Introduction: Primary tumors arising from the small bowel are a rarity among GI cancers. Here we explore the path to a diagnosis of duodenal adenocarcinoma.
Case Description/Methods: A 65-year-old male with a history of diverticulosis and DVTs presented with a 3-day history of painless melena. Previously, he had separately presented with stable hematochezia, and with extensive lower extremity DVTs and saddle PE needing anticoagulation. In both cases, outpatient follow up for colonoscopy was advised. In the present case, the patient presented with a hemoglobin of 7.8 (previous 13.7), Alkaline Phosphatase of 188, AST 38 and ALT 61. A CT angiogram did not reveal a source.
GI performed an EGD which demonstrated an infiltrative and fungating circumferential 40 mm mass in the second part of the duodenum that eroded through the wall (Figure). Biopsies showed grade G2 moderately differentiated adenocarcinoma. MRI abdomen confirmed a duodenal mass with extension to the pancreatic head and encasement of the common bile duct.
Surgery took the patient for a Whipple's procedure. Intraoperative biopsies demonstrated moderately differentiated duodenal adenocarcinoma with metastasis in 6 out of 20 nodes. After discharge the patient was started on adjuvant FOLFOX chemotherapy for 3 months and continues to do well and follow up with oncology.
Discussion: Of primary small bowel tumors adenocarcinoma is the second most common, representing around 30-40% of small bowel cancers. Within the duodenum, tumors are most likely to arise in the second section, near the ampulla.
Due to nonspecific symptoms most of these tumors are diagnosed at later stages. Tumors near the ampulla present earlier with biliary obstruction. Patients can present with abdominal pain, weight loss, jaundice, vomiting and less commonly GI bleed. Studies show that patients have a median life expectancy of 5.7 months following diagnosis.
Treatment for these cancers is contingent on TMN staging. If caught early the cancerous tissue can be removed by endoscopic resection. With more extensive disease in the first or second portion of the duodenum treatment requires full pancreaticoduodenectomy. For those with a tumor in the third or fourth portion a segmental duodenectomy is preferred. The use of chemotherapy after surgery remains controversial with poor evidence of mortality benefit.
It is vital in patients with nonspecific symptoms and no clear etiology to rule out small bowel cancers in order to improve their overall chance of survival.
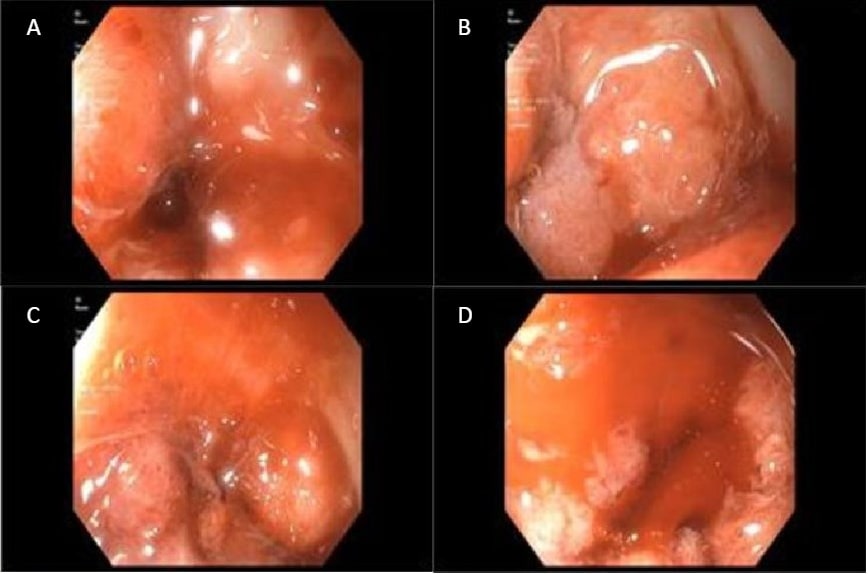
Figure: Photos captured during EGD. A & B showing mass in the second portion of the duodenum. C & D showing bleeding after biopsy of mass.
Disclosures:
Sarah Elrod indicated no relevant financial relationships.
Kyle Marrache indicated no relevant financial relationships.
Zulfiqar Arif indicated no relevant financial relationships.
Sarah Elrod, DO1, Kyle Marrache, DO1, Zulfiqar Arif, MD2. B0679 - Initial Presentation of Primary Duodenal Adenocarcinoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.