Avleen Kaur, MD1, Sadat Iqbal, MD2, Kunal Patel, MD3, Linda Lee, MD1, Anna Fomitchova, MD4 1Maimonides Health, Brooklyn, NY; 2Maimonides Medical Center, Brooklyn, NY; 3Saint Peter's University Hospital, New Brunswick, NJ; 4State University of New York Downstate, Brooklyn, NY
Introduction: Malignant pericardial effusion is common, reported in 5–15% of cancer patients. It most commonly arises from metastasis of lymphomas and tumors of the lung, breast, and, infrequently, the gastrointestinal tract. We report a rare case of metastatic colon cancer without the direct involvement of other solid organs suggesting a lymphatic spread.
Case Description/Methods: A 28-year-old man presented with one day of sudden onset of shortness of breath at rest. Vitals were significant for tachycardia. On examination, the lungs were clear to auscultation with distant heart sounds; the abdomen was soft without tenderness. The clinical presentation was suggestive of pericardial effusion. Laboratory studies revealed microcytic anemia with hemoglobin of 11.7 g/dl. CT angiography chest with contrast revealed moderate to large PEff and subsegmental pulmonary embolism. An ECHO showed large PEff, without any signs of tamponade. He underwent video-assisted thoracoscopic surgery for PEff with a pericardial window. The mediastinal lymph node biopsy and pericardial fluid cytology showed metastatic adenocarcinoma cells. A CT scan of the chest/abdomen/pelvis was performed to find the primary malignancy, which revealed a segmental thickening of the proximal ascending colon and ileum with proximal cecal distension, lymphadenopathy, without liver metastasis. A CF showed a large polypoidal mass in the ascending colon, and biopsy revealed poorly differentiated adenocarcinoma in ascending colon. He was started on palliative chemotherapy with capecitabine, oxaliplatin, and bevacizumab and was discharged with outpatient oncology follow-up.
Discussion: Colorectal cancer (CRC) is the third most common cancer in the United States. It primarily spreads hematogenous via the portal venous system that drains the colon and proximal rectum to the liver and the lungs to the heart. However, cardiac metastasis is rare. In our patient, we assume lymphatic spread of colon cancer due to isolated pericardial involvement in the absence of solid organ involvement. To our knowledge, this is the second reported case of lymphatic spread of colon cancer. Therefore, we emphasize considering pericardial effusions as a marker of occult malignancy to facilitate rapid diagnosis and prompt treatment. However, the prognosis for carcinomatous pericarditis is poor, with a 2-5 months median survival.
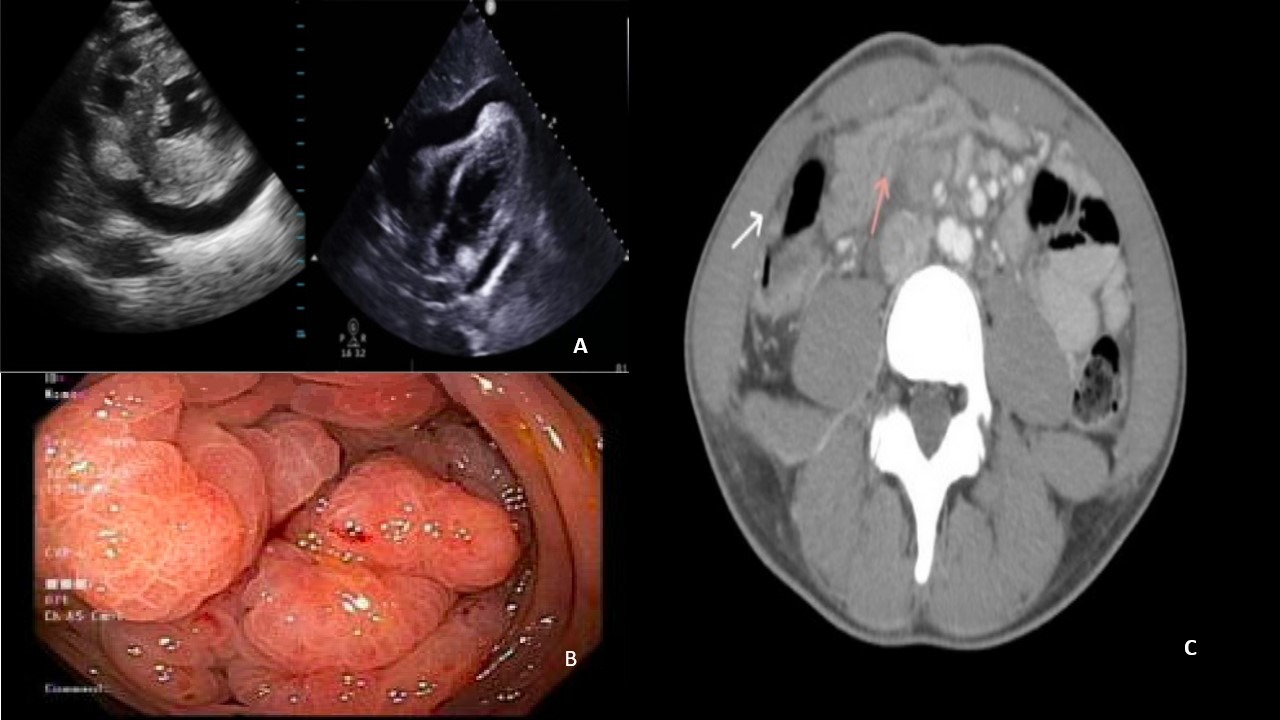
Figure: Figure 1: A-Echocardiogram: Parasternal short axis view showing large pericardial effusion, no signs of cardiac tamponade. B-Colonoscopy showing a lobulated mass in cecum. C-Computed Tomography (C.T.) scan with PO/IV contrast showing mass vs segmental inflammation in proximal ascending colon (pink arrow). Mild thickening of terminal ileum (white arrow).
Disclosures:
Avleen Kaur indicated no relevant financial relationships.
Sadat Iqbal indicated no relevant financial relationships.
Kunal Patel indicated no relevant financial relationships.
Linda Lee indicated no relevant financial relationships.
Anna Fomitchova indicated no relevant financial relationships.
Avleen Kaur, MD1, Sadat Iqbal, MD2, Kunal Patel, MD3, Linda Lee, MD1, Anna Fomitchova, MD4. A0137 - Isolated Cardiac Metastasis as an Initial Presentation of Colorectal Cancer in a Young Male Due to Lymphatic Spread, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.