Medstar Georgetown University Hospital Washington, DC
Sara Kiparizoska, MD, Mark Real, MD, Stanley Benjamin, MD, Norio Azumi, MD Medstar Georgetown University Hospital, Washington, DC
Introduction: Leiomyosarcoma (LMS) is an aggressive soft tissue tumor that is rarely found in the gastrointestinal (GI) tract. Commonly misdiagnosed as a gastrointestinal stromal tumor (GIST), LMS incidence is now more accurately identified and rarer than previously thought due to advances in immunohistochemical (IHC) staining over the last 20 years. LMS can be distinguished from GIST by its distinctive IHC staining positive for smooth muscle actin (SMA) and desmin and negative for markers CD117, CD34, DOG1. We present the case of a patient who was found to have a colonic polyp with increased mitotic activity and ultimately diagnosed with metastatic LMS.
Case Description/Methods: A 72 year old woman with history of uterine fibroids post hysterectomy underwent a routine screening colonoscopy. She was found to have a diminutive polyp in the hepatic flexure identified as a smooth muscle neoplasm with increased mitotic activity. A follow up colonoscopy 6 months later also revealed a polyp with smooth muscle neoplasm with high mitotic activity (2-3 per one high-power field). IHC staining on both polyps showed positive SMA and negative GIST markers. Proliferation index (Ki-67) was 20%. The differential diagnosis was rare primary leiomyosarcoma of colon versus metastasis.
Abdominal and pelvis imaging with CT and MRI was nonrevealing. Three months after the follow up colonoscopy, the patient had ongoing neck pain and was found to have a lung mass and bone metastasis identified as LMS. She received multiple chemotherapy agents and then anastrozole after tumor hormone staining was estrogen receptor positive.
Discussion: We present an interesting case of metastatic leiomyosarcoma involving colon, lung, and bone with unknown primary. Because LMS spreads hematogenously, it is difficult to identify the primary LMS lesion. Her history of uterine leiomyoma is another potential source. Initial expert consultation indicated primary smooth muscle neoplasm of colon with 40% chance of progression. It became clear due to the discovery of additional foci of metastasis that the colonic lesions were also metastasis.
We share this case to highlight a constellation of overlapping characteristics of mesenchymal tumors in the GI tract. The distinction among LMS and GIST with proper IHC staining is extremely important since treatment is vastly different. If the diagnosis is not immediately clear, like in our case, expert pathology evaluation, a multidisciplinary approach, and close endoscopic follow up are of the upmost importance.
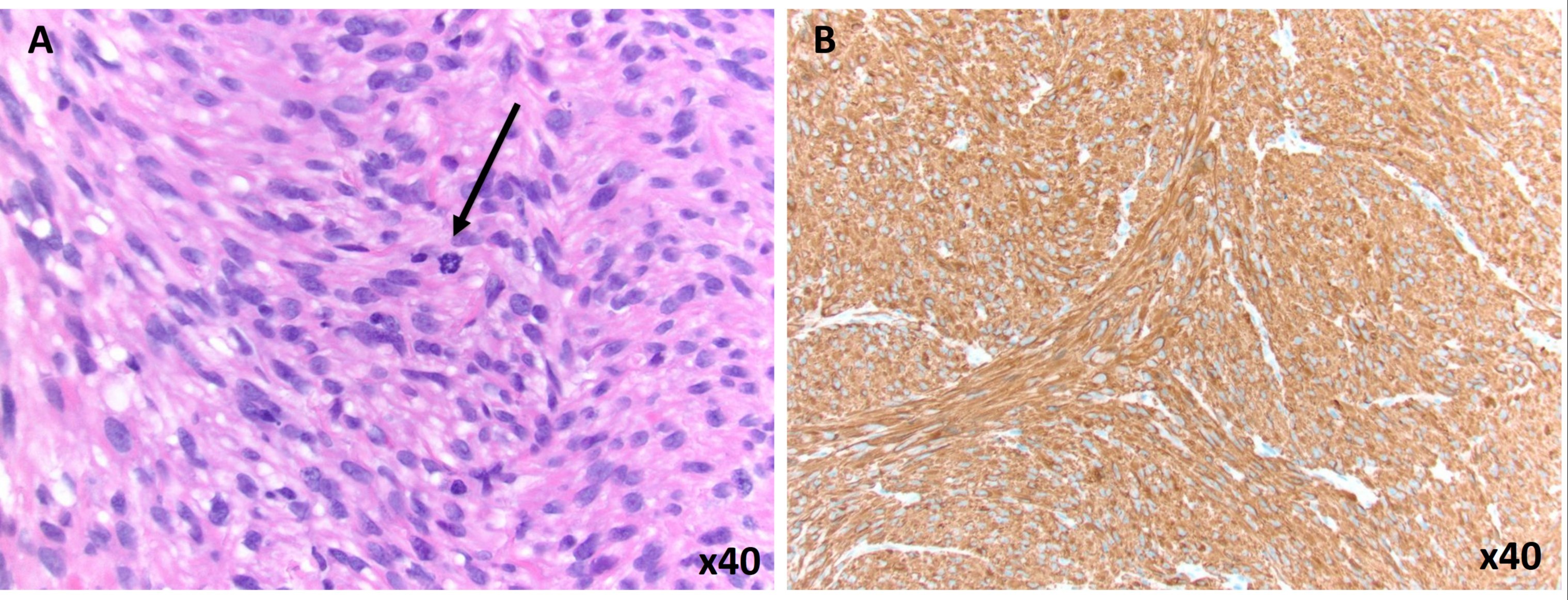
Figure: Figure 1: High magnification pathology slides. (A) Mitotic figure identified by arrow. (B) IHC staining confirms the smooth muscle nature of this neoplasm as tumor cell are positive for SMA.
Disclosures:
Sara Kiparizoska indicated no relevant financial relationships.
Mark Real indicated no relevant financial relationships.
Stanley Benjamin indicated no relevant financial relationships.
Norio Azumi indicated no relevant financial relationships.
Sara Kiparizoska, MD, Mark Real, MD, Stanley Benjamin, MD, Norio Azumi, MD. B0125 - A Rare Case of Primary Leiomyosarcoma of the Colon versus Metastasis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.