Rewanth Katamreddy, MD1, SuLin Lim, MD1, Saraswathi Lakkasani, MD2, Sowjanya Kalluri, MBBS1, Gunwant Guron, MBBS1, Yatinder Bains, MD2 1Saint Michael's Medical Center, Newark, NJ; 2Saint Michael's Medical Center, New York Medical College, Newark, NJ
Introduction: The incidence of extra-nodal NHL is 25%. The Gastrointestinal (GI) tract is the most common extra-nodal site accounting for 30-40 % of extra-nodal NHL. GI lymphomas can be in the stomach (65%), small intestine (20%–30%), colon (10%–20%), and esophagus (< 1%). Here we are presenting a case of intestinal lymphoma presented with obstructive Jaundice.
Case Description/Methods: A 79-year-old woman with a past medical history of HIV on treatment presented with abdominal pain, loss of appetite, and weight loss of 15 kg over a period of one year. Labs showed total bilirubin of 5.6 mg/dl and direct bilirubin of 3.12 mg/dl. Imaging showed dilated CBD measuring 1.8 cm, neoplastic mass in the cecum. MRI showed dilated common bile duct and abnormal ampullary area. The patient underwent upper Endoscopy which showed a mass at the major papilla. Biopsy of the mass is positive for CD45 with Ki-67 80% consistent with Diffuse large B cell Lymphoma (DLBCL). Colonoscopy revealed multiple malignant polypoid lesions in the cecum, ascending colon, hepatic flexure, transverse colon, and rectum with biopsy of all lesions consistent with DLBCL. Immunohistochemical analysis confirms the presence of a malignant B-cell lymphoma diffusely positive for CD20, CD79a, BCL-2, BCL6, MUM-1, and c-MYC with a high Ki and positive for cyclin D1. Bone marrow biopsy showed no evidence of lymphoma. Biliary decompression with a metallic stent was done under CT guidance. Dose adjusted mini-CHOP treatment was administered under close monitoring. Eventually, the patient deceased due to non-response and hemodynamic instability.
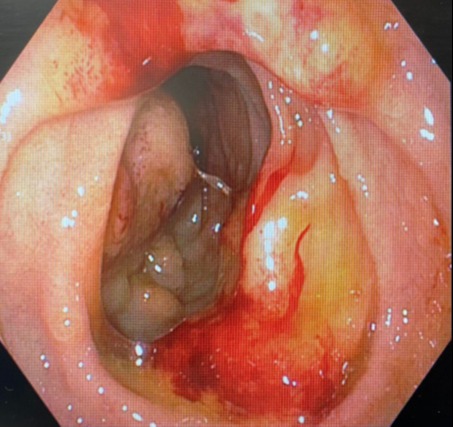
Discussion: GI lymphomas can present with many manifestations but, obstructive jaundice is rare. We noticed the fungating mass around the ampulla our suspicion was a periampullary carcinoma. Colonoscopy revealed multiple masses and various locations, which lead us to consider a differential of carcinoid tumors. However, to our surprise biopsy revealed diffuse large B cell lymphoma as it accounts for only 1-2% of all GI malignancies. Obstructive jaundice occurs in 1-2 % of the cases of non-Hodgkin’s lymphoma, which is mostly due to peri-hilar and peri-portal lymphadenopathy. This case is a rare finding due to intraluminal lymphoma causing distal biliary obstruction. Our patient is a rare finding as lymphoma has occurred even after risk mitigation for HIV. Standard treatment is a combination of chemo-immunotherapy (RCHOP)with excellent survival rates. Without therapy, the survival times are limited to a few months.
Figure: Fungating mass around the Ampulla
Disclosures:
Rewanth Katamreddy indicated no relevant financial relationships.
SuLin Lim indicated no relevant financial relationships.
Saraswathi Lakkasani indicated no relevant financial relationships.
Sowjanya Kalluri indicated no relevant financial relationships.
Gunwant Guron indicated no relevant financial relationships.
Yatinder Bains indicated no relevant financial relationships.
Rewanth Katamreddy, MD1, SuLin Lim, MD1, Saraswathi Lakkasani, MD2, Sowjanya Kalluri, MBBS1, Gunwant Guron, MBBS1, Yatinder Bains, MD2. B0026 - A Case of Gastrointestinal Lymphoma Presented as Obstructive Jaundice, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.