Monica Huynh, DO1, Liza Plafsky, MD2, Ali Zakaria, MD2, Shreya Narayanan, MD3, Krishen Patel, MD2, Jennifer Seminerio-Diehl, MD2, Ali Abbas, MD2 1Nova Southeastern University, Largo, FL; 2University of South Florida, Tampa, FL; 3University of South Florida Morsani College of Medicine, Tampa, FL
Introduction: Achalasia is a rare esophageal motility disorder characterized by progressive dysphagia to solids and eventually liquids[1-2]. Pseudoachalasia refers to an achalasia secondary to an underlying etiology, such as masses, post-operative complications, or paraneoplastic syndromes[1-2]. The most common cause of pseudoachalasia is adenocarcinoma of the cardia or esophagus [1] however, we discuss a rare case that deviates from the typical etiology of esophageal cancer.
Case Description/Methods: This is a 71 year-old male presenting with intermittent dysphagia for years with rapid progression for a month including intolerance of oral intake and six-pound weight loss. On examination he was hemodynamically stable with a soft, nontender abdomen.
His initial barium esophagram revealed decreased esophageal peristalsis, esophageal distention, and narrowing at the gastroesophageal junction (GEJ) with “bird beak” appearance consistent with possible achalasia. Further imaging studies were performed with computed tomography (CT), esophagogastroduodenoscopy (EGD) with dilation, and endoscopic ultrasound with biopsies revealing an invasive squamous cell carcinoma of the GEJ with submucosal involvement extending into the gastric cardia.
We present our patient as the first reported case of pseudoachalasia due to SCC of the GEJ. The patient underwent esophageal stenting and mediport placement with plans for neoadjuvant chemotherapy with concurrent radiotherapy followed by definitive resection.
Discussion: Pseudoachalasia is often misdiagnosed for primary achalasia because of its rarity, indistinguishable symptomatology, and normal findings on CT, EGD, and biopsy[1-2]. Nearly 75% of pseudoachalasia cases are due to adenocarcinoma of the gastric cardia[1]. Only one case of pseudoachalasia has been known to be caused by SCC in the distal esophagus[3]. SCC of the GEJ is an extremely rare esophageal malignancy and has never previously been reported as an underlying cause of pseudoachalasia.
References
Campo SM, Zullo A, Scandavini CM, Frezza B, Cerro P, Balducci G. Pseudoachalasia: A peculiar case report and review of the literature. World J Gastrointest Endosc. 2013;5(9):450-454.
Roushan N, Zolfaghari A, Asadi M, Taslimi R. Pseudoachalasia: a diagnostic challenge. Med J Islam Repub Iran. 2014;28:54.
Kahrilas, P., Kishk, S., Helm, J., Dodds, W., Harig, J. and Hogan, W., 1987. Comparison of pseudoachalasia and achalasia. The American Journal of Medicine. 1987;82(3):439-446.
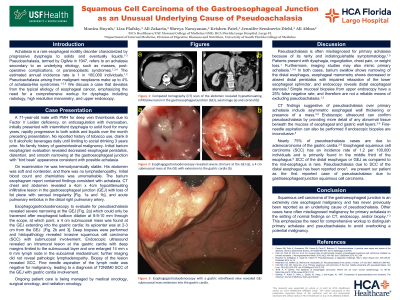
Figure: Esophagogastroduodenoscopy revealed severe stricture at the GEJ with a 4 cm submucosal mass at the GEJ with extension to the gastric cardia.
Disclosures:
Monica Huynh indicated no relevant financial relationships.
Liza Plafsky indicated no relevant financial relationships.
Ali Zakaria indicated no relevant financial relationships.
Shreya Narayanan indicated no relevant financial relationships.
Krishen Patel indicated no relevant financial relationships.
Jennifer Seminerio-Diehl indicated no relevant financial relationships.
Ali Abbas indicated no relevant financial relationships.
Monica Huynh, DO1, Liza Plafsky, MD2, Ali Zakaria, MD2, Shreya Narayanan, MD3, Krishen Patel, MD2, Jennifer Seminerio-Diehl, MD2, Ali Abbas, MD2. C0239 - Squamous Cell Carcinoma of the Gastroesophageal Junction as an Unusual Underlying Cause of Pseudoachalasia, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.