Introduction: Statins are commonly used to prevent cardiovascular disease. However, a small subset of patients may develop autoimmune myopathy, a form of inflammatory myositis characterized by proximal muscle weakness and in some cases, dysphagia. We present two cases highlighting statin-induced necrotizing autoimmune myopathy (SINAM), a rare entity affecting roughly 2 cases per 1 million people.
Case Description/Methods: Two Hispanic men, aged 60 and 71, presented with dysphagia and transaminitis. They reported gradual onset of proximal muscle weakness and weight loss and were taking atorvastatin 20mg and 80mg, respectively.
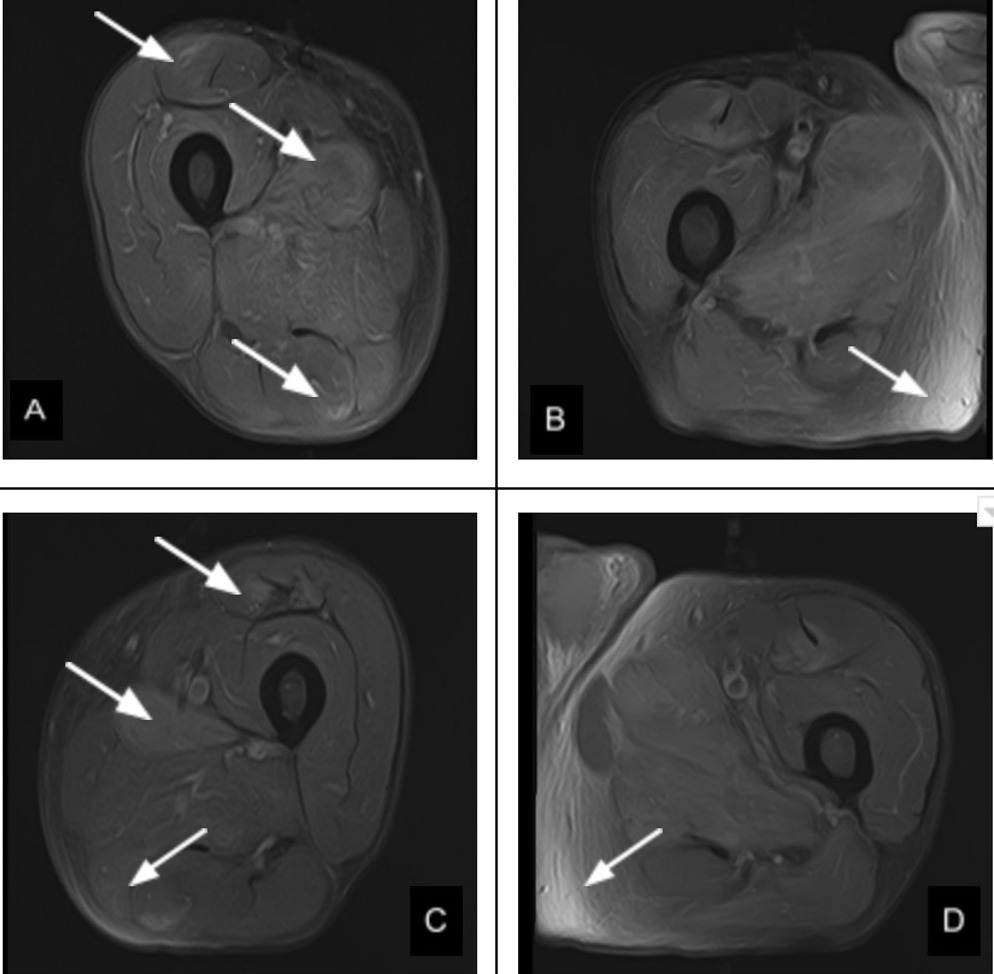
Case 1: Labs revealed ALP 58 IU/L, AST 238 U/L, ALT 407 U/L, CK 7228 U/L, normal CRP, ESR, and HMG CoA reductase (HMGCR) antibodies 257 U/mL. EGD was unrevealing. MRI of the pelvis/femur showed patchy, symmetric intramuscular edema in leg muscles (Figure 1). Muscle biopsy revealed myonecrosis consistent with immune-mediated necrotizing myopathy.
Case 2: Labs revealed ALP 79 IU/L, AST 571 U/L, ALT 373 U/L, CK 8392 U/L, CRP 19.2 mg/L, ESR 67 mm/hr, and HMGCR antibodies 367 U/mL. Muscle biopsy was not pursued. Both cases revealed negative viral hepatitis, ANA, myositis panel, smooth muscle Ab, LKM-1 Ab, total IgG, ferritin, anti-mitochondrial Ab, and alpha-1 antitrypsin.
Both patients were started on high-dose steroids. Case 1 patient had minimal improvement and was subsequently started on mycophenolate and rituximab. He remains under close monitoring. Case 2 patient had persistent severe weakness and dysphagia, therefore intravenous immunoglobulin (IVIG) and mycophenolate were added. However, dysphagia persists despite a consistent decrease in muscle enzymes. He remains hospitalized and is pending PEG tube placement.
Discussion: SINAM is a rare variant of idiopathic inflammatory myopathy characterized by proximal muscle weakness and myofiber necrosis after statin exposure. Diagnosis is made with positive antibodies to HMGCR and may avoid the need for muscle biopsy in the appropriate clinical context. Cessation of statin and initiation of glucocorticoids are first-line treatments. However, many cases are refractory to steroid monotherapy. Other therapies such as IVIG and immunosuppressants serve a role in refractory disease. Alternative lipid-lowering agents should be used, and statins must not be rechallenged. These cases emphasize that muscle weakness, dysphagia and transaminitis should be evaluated diligently as early recognition can lead to initiation of life-saving treatment.
Figure: Figure 1: A-D. MRI pelvis/femur showing bilateral patchy and symmetric intramuscular edema in leg muscles.
Disclosures:
Hunza Chaudhry indicated no relevant financial relationships.
Joanne Lin indicated no relevant financial relationships.
Rameen Atefi indicated no relevant financial relationships.
Jeffrey Hagino indicated no relevant financial relationships.
Candice Reyes indicated no relevant financial relationships.
Marina Roytman indicated no relevant financial relationships.
Hunza Chaudhry, MD1, Joanne Lin, DO2, Rameen Atefi, DO2, Jeffrey Hagino, DO2, Candice Reyes, MD2, Marina Roytman, MD2. C0572 - A Tough Pill to Swallow: A Case Series of Statin-Induced Necrotizing Autoimmune Myopathy Manifesting as Dysphagia and Transaminitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.