Saint Joseph's University Medical Center Paterson, NJ
Ariana R. Tagliaferri, MD1, Nida Ansari, DO2, Yana Cavanagh, MD1 1Saint Joseph's University Medical Center, Paterson, NJ; 2St. Joseph's Regional Medical Center, Paterson, NJ
Introduction: Congenital Gallbladder Agenesis (CGA) is a rare anomaly of the biliary tract with an annual incidence of 0.007%. Most patients are asymptomatic but can present with biliary colic and are subsequently misdiagnosed with gallstones. Cholangiocarcinoma (CCA) is a malignant tumor arising from the biliary ducts in patients with underlying chronic biliary tract inflammation, PSC or other diseases. Few studies have reported recurrent cholelithiasis in CGA, but there is only one known case of concomitant CCA and CGA. Herein we present a 79 YO M who presented with recurrent gallstones and was diagnosed with gallbladder agenesis intraoperatively with pathology consistent with cholangiocarcinoma.
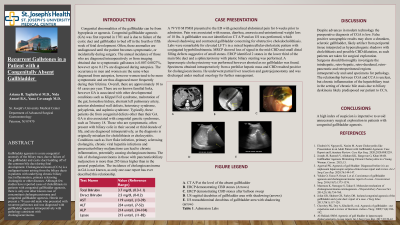
Case Description/Methods: A 79 YO M PMH presented to the ED with generalized abdominal pain for 6 weeks prior to admission. Pain was associated with nausea, diarrhea, anorexia and unintentional weight loss of 18 lbs. A gallbladder was not identified on CT A/P and an US was performed, which showed shadowing and contracted gallbladder concerning for obstructive choledocholithiasis. Labs were remarkable for elevated LFT’s in a mixed hepatocellular-cholestatic pattern with conjugated hyperbilirubinemia. MRCP showed loss of signal in the mid-CBD and small distal filling defects suggestive of small stones. ERCP identified 2 stones in the lower third of the main bile duct and a sphincterotomy with plastic biliary stenting was performed. A laparoscopic cholecystectomy was performed however aborted as no gallbladder was found. Specimens obtained intraoperatively from a perihilar hepatic mass and CBD resulted positive for cholangiocarcinoma. He underwent partial liver resection and gastrojejunostomy and was discharged under medical oncology for further management.
Discussion: Despite advances in modern technology the preoperative diagnosis of CGA is low. False positive sonographic results may show a shrunken, sclerotic gallbladder, likely artifact from periportal tissue interpreted as hyperechogenic shadows with cholelithiasis and possible CBD dilatation, as such patients are taken for surgical exploration. Surgeons should thoroughly investigate the intrahepatic, retro-hepatic, retro-duodenal, retro-pancreatic and retroperitoneal regions intraoperatively and send specimens for pathology. The relationship between CGA and CCA is unclear, but chronic inflammation of the hepatobiliary tract in the setting of chronic bile stasis due to biliary dyskinesia likely predisposed our patient to CCA.
Disclosures:
Ariana Tagliaferri indicated no relevant financial relationships.
Nida Ansari indicated no relevant financial relationships.
Yana Cavanagh indicated no relevant financial relationships.
Ariana R. Tagliaferri, MD1, Nida Ansari, DO2, Yana Cavanagh, MD1. A0048 - Recurrent Gallstones in a Patient With a Congenitally Absent Gallbladder and Cholangiocarcinoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.