University of Texas Health Science Center San Antonio, TX
Hamza I. Khan, MD1, Muhammad Haris, MD2, Juan Echavarria, MS, MD2, Chandraprakash Umapathy, MD2 1University of Texas Health Science Center, San Antonio, TX; 2University of Texas Health San Antonio, San Antonio, TX
Introduction: Neoplasms of the duodenum account for a fraction of overall gastrointestinal tumors. Even when a lesion is found in the duodenum, it is more likely to be of secondary neoplastic origin than primary. Here we present a unique case of primary renal cell carcinoma (RCC) diagnosed on EGD.
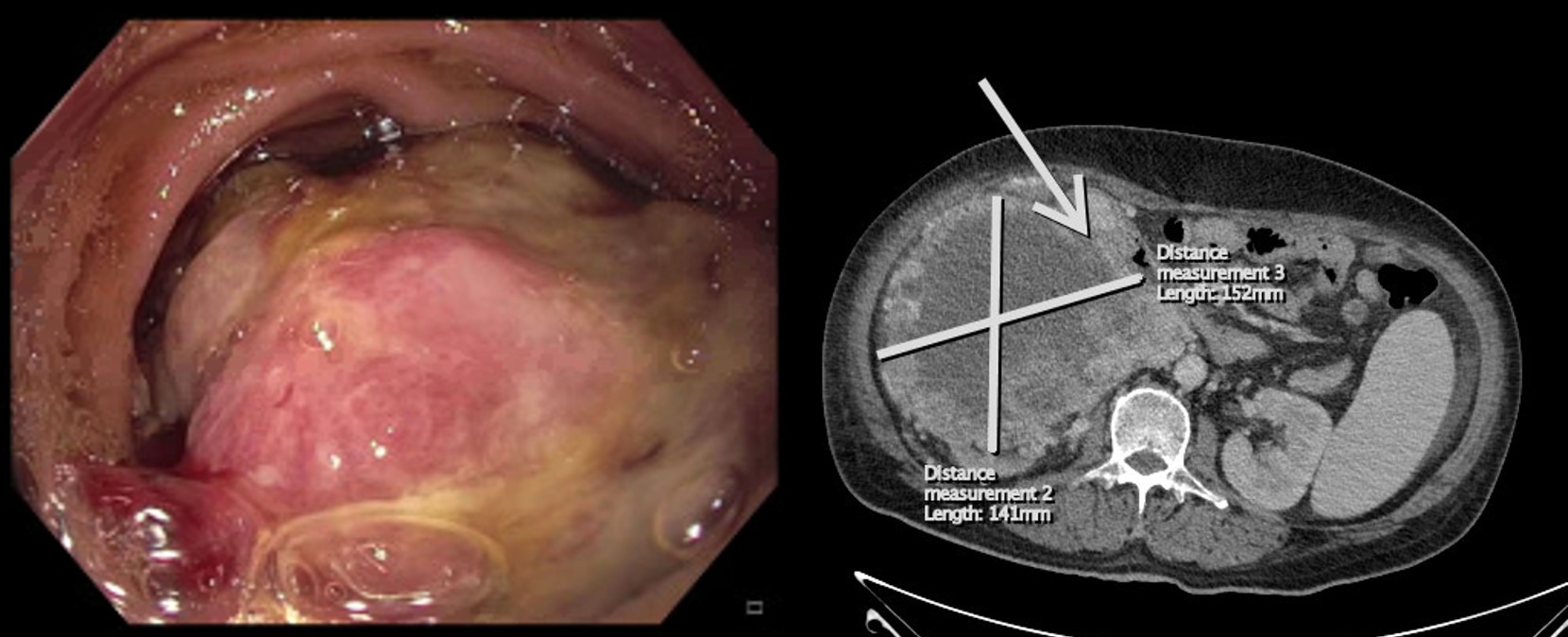
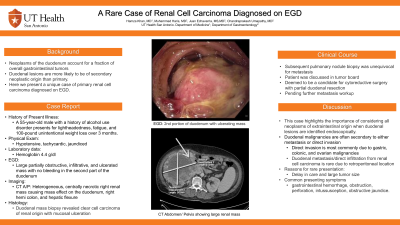
Case Description/Methods: A 55-year-old male with a history of alcohol use disorder presented to the emergency department for lightheadedness, fatigue, and 100-pound unintentional weight loss over 3 months. On exam, the patient was found to be hypotensive, tachycardic, and jaundiced. Laboratory values were pertinent for a Hemoglobin of 4.4 g/dl. After adequate resuscitation, esophagogastroduodenoscopy (EGD) was performed that showed a large partially obstructive, infiltrative, and ulcerated mass with no bleeding in the second part of the duodenum. Histology from the duodenal mass biopsy revealed clear cell carcinoma of renal origin with mucosal ulceration. An abdominal computerized tomography (CT) scan showed a heterogeneous, centrally necrotic right renal mass causing mass effect on the second and third portions of the duodenum, right hemicolon, and hepatic flexure. The scan was also suggestive of duodenal invasion by the mass. Solid pulmonary nodule biopsy was unequivocal for metastasis. The patient was discussed in tumor board and deemed to be a candidate for cytoreductive surgery with partial duodenal resection and systemic immunotherapy if metastasis was confirmed on future biopsies.
Discussion: Duodenal metastasis from RCC is very rare and poses a diagnostic challenge. The most common presentation is with upper gastrointestinal hemorrhage or obstruction, though sometimes it can present with perforation, intussusception, or obstructive jaundice. Duodenal involvement is often from direct infiltration or metastatic spread. Delay in care and large tumor size are the likely reasons for the rare presentation seen in this patient. This case highlights the importance of considering all neoplasms of extraintestinal origin when duodenal lesions are identified endoscopically.
Figure: Figure1: 2nd portion of duodenum. Figure 2: CT Abdomen/Pelvis
Disclosures:
Hamza Khan indicated no relevant financial relationships.
Muhammad Haris indicated no relevant financial relationships.
Juan Echavarria indicated no relevant financial relationships.
Chandraprakash Umapathy indicated no relevant financial relationships.
Hamza I. Khan, MD1, Muhammad Haris, MD2, Juan Echavarria, MS, MD2, Chandraprakash Umapathy, MD2. A0282 - A Rare Case of Renal Cell Carcinoma Diagnosed on EGD, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.

.jpg "Hamza I. Khan, MD photo")