Farah Heis, MBBS, Ahmad Al-Alwan, MD, Harshil Fichadiya, MBBS, Raghu Tiperneni, MD Monmouth Medical Center, Long Branch, NJ
Introduction: Duodenal diverticulum is a frequent and common asymptomatic incidental finding and is commonly located at the second part of the duodenum. However, complications have been reported such as inflammation of the diverticulum, hemorrhage and perforation. Its presentation can mimic arrays of abdominal pathologies. In our case, patient presented with epigastric pain similar to the presentation of acute pancreatitis.
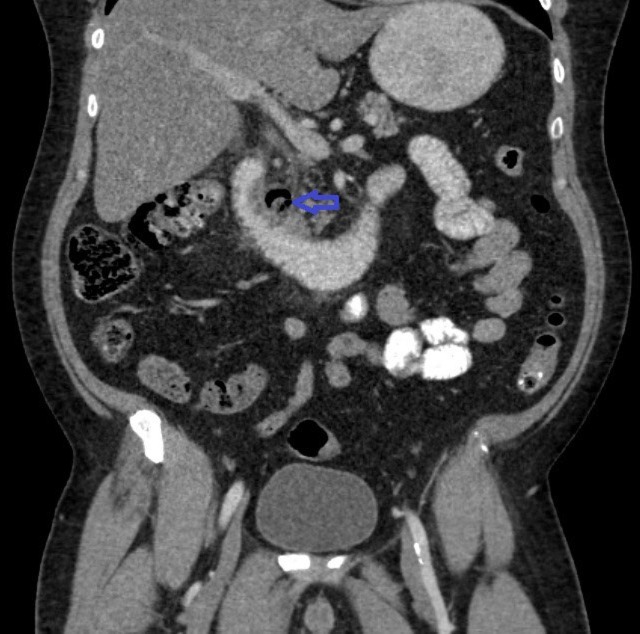
Case Description/Methods: Patient is a 52 yo male with medical history of type 2 DM and hypertension who presented to the ED for epigastric pain for two days duration. It was a sudden onset moderate progressive stabbing epigastric abdominal pain radiating to the back, associated with nausea, however patient denies vomiting, changes in bowel habits, fever, or chills. Upon arrival to the ED, his vital signs were within normal limits, his blood work demonstrated leukocytosis of 11.8 K/CMM, Hb 13.3 g/dL with MCV of 80 fL and CMP values were within normal limits. Blood cultures showed no evidence of microorganisms, he had an US of the abdomen which showed hepatic steatosis and hepatomegaly with no evidence of cholecystitis, chest X-Ray was also done which had unremarkable findings. Further radiological studies were ordered including CT abdomen and pelvis with contrast (Figure 1) which had significant findings of inflammatory changes in the second portion of the duodenum in the setting of duodenal diverticulum, so the patient was admitted for management of duodenal diverticulitis and was started on Flagyl IV 500mg every 8 hour interval and Ciprofloxacin IV 400mg daily for one day and then antibiotics were changed to Unasyn 3g every 6 hour interval. Patient’s abdominal pain resolved after 4 days of antibiotics. He had an EGD which showed small erosion in the antrum as well as mild duodenitis with diverticular deformity, no ulcers or masses were noted in the duodenum. Prior to discharge, MRI of the abdomen was ordered which showed duodenal diverticulitis that was regressing compared to prior CT study. Patient was discharged home with a follow up with a gastroenterologist two weeks after discharge.
Discussion: Duodenal diverticulitis is a possible differential diagnosis in acute abdominal pain. It is diagnosed with computed tomography showing inflammatory changes in duodenal diverticulum and managed medically with antibiotics covering gram negative bacteria as with our patient, however if complications like perforation occur, more aggressive interventions should be taken.
Figure: Figure 1: CT abdomen and pelvis with contrast showing significant inflammatory changes in the second portion of the duodenum in the setting of duodenal diverticulum.
Disclosures:
Farah Heis indicated no relevant financial relationships.
Ahmad Al-Alwan indicated no relevant financial relationships.
Harshil Fichadiya indicated no relevant financial relationships.
Raghu Tiperneni indicated no relevant financial relationships.
Farah Heis, MBBS, Ahmad Al-Alwan, MD, Harshil Fichadiya, MBBS, Raghu Tiperneni, MD. B0660 - Duodenal Diverticulitis Mimicking Acute Pancreatitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.